Omvoh (mirikizumab-mrkz) injection, solution
1 INDICATIONS AND USAGE
OMVOH is indicated for the treatment of:
- moderately to severely active ulcerative colitis in adults.
- moderately to severely active Crohn's disease in adults.
2 DOSAGE AND ADMINISTRATION
Prior to Treatment Initiation
- Evaluate patients for tuberculosis (TB) infection. (2.1, 5.3)
- Obtain liver enzymes and bilirubin levels. (2.1, 5.4)
- Complete all age-appropriate vaccinations according to current immunization guidelines. (2.1, 5.5)
Recommended Dosage for Ulcerative Colitis
- Induction Dosage: Week 0, Week 4, and Week 8: Infuse 300 mg intravenously over at least 30 minutes. (2.2)
- Maintenance Dosage: Week 12 and every 4 weeks thereafter: Inject 200 mg subcutaneously (given as either one injection of 200 mg or as two consecutive injections of 100 mg each). (2.2)
Recommended Dosage for Crohn's Disease
- Induction Dosage: Week 0, Week 4, and Week 8: Infuse 900 mg intravenously over at least 90 minutes. (2.3)
- Maintenance Dosage: Week 12 and every 4 weeks thereafter: Inject 300 mg subcutaneously (given as two consecutive injections of 100 mg and 200 mg in any order). (2.3)
Preparation and Administration Instructions
2.1 Recommended Evaluations and Immunizations Prior to Treatment Initiation
- Evaluate patients for tuberculosis (TB) infection prior to initiating treatment with OMVOH [see Warnings and Precautions (5.3)].
- Obtain liver enzymes and bilirubin levels prior to initiating treatment with OMVOH [see Warnings and Precautions (5.4)].
- Complete all age-appropriate vaccinations according to current immunization guidelines [see Warnings and Precautions (5.5)].
2.2 Recommended Dosage for Ulcerative Colitis
Induction Dosage
Week 0, Week 4, and Week 8: Infuse 300 mg intravenously over at least 30 minutes [see Dosage and Administration (2.4)].
2.3 Recommended Dosage for Crohn's Disease
Induction Dosage
Week 0, Week 4, and Week 8: Infuse 900 mg intravenously over at least 90 minutes [see Dosage and Administration (2.4)].
2.4 Preparation and Administration Instructions for Intravenous Infusion
- OMVOH for intravenous use is intended for administration by a healthcare provider using aseptic technique.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. The solution should be a clear to opalescent, colorless to slightly yellow to slightly brown solution, and free of visible particles. Do not use OMVOH if it is cloudy or there are visible particles.
- Prior to intravenous administration, determine the dose needed based on the patient's indication (see Table 1 below). For Crohn's disease, discard 45 mL of the infusion bag prior to adding vial contents. Withdraw the required amount of solution from the vial(s) using a 18 gauge to 21 gauge needle and transfer to an infusion bag containing 0.9% Sodium Chloride Injection or 5% Dextrose Injection (see Table 1 below). Do not mix with other drugs. Do not dilute or infuse through the same intravenous line with other solutions.
- Gently invert the infusion bag to mix the contents. Do not shake the prepared infusion bag.
- Connect the intravenous administration set (infusion line) to the prepared infusion bag and prime the line.
- Infuse the diluted solution intravenously over a period of at least 30 minutes for the 300 mg dose; at least 90 minutes for the 900 mg dose. If stored refrigerated, allow the diluted solution in the infusion bag to warm to room temperature prior to the start of the intravenous infusion.
- At the end of the infusion, flush the line with 0.9% Sodium Chloride Injection or 5% Dextrose Injection.
- Administer the flush at the same infusion rate as used for OMVOH administration.
- The time required to flush OMVOH solution from the infusion line is in addition to the minimum 30-minute infusion time.
Storage of Diluted Solution
- Start the infusion immediately after preparation. If not used immediately, store the diluted infusion solution in the refrigerator at 2°C to 8°C (36°F to 46°F). Use the diluted infusion solution within 48 total hours, of which not more than 5 hours are permitted at non-refrigerated temperatures not to exceed 25°C (77°F), starting from the time of vial puncture.
- Keep drug product away from direct heat or light. Do not freeze the diluted solution in the prepared infusion bag.
2.5 Preparation and Administration Instructions for Subcutaneous Injection
- OMVOH is intended for use under the guidance and supervision of a healthcare professional. Patients may self-inject OMVOH after training in subcutaneous injection technique. Provide proper training to patients and/or caregivers on the subcutaneous injection technique of OMVOH according to the “Instructions for Use”, included with the packaged product.
- Before injection, remove OMVOH prefilled pens or OMVOH prefilled syringes from the refrigerator, and leave at room temperature for 45 minutes.
- Do not shake the prefilled pens or prefilled syringes.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. The solution should be a clear to opalescent, colorless to slightly yellow to slightly brown solution, and free of visible particles. Do not use OMVOH if it is cloudy, discolored, or there are visible particles.
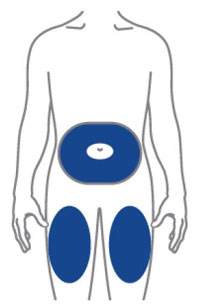
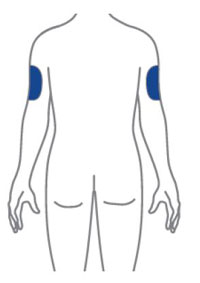
- Sites for injection include the abdomen, thigh, and back of the upper arm. Instruct patients to inject in a different location (such as upper arms, thighs or any quadrant of abdomen) than the previous injection. Administration of OMVOH in the back of upper arm may only be performed by another person.
- Do not inject into areas where the skin is tender, bruised, erythematous, or indurated.
- OMVOH does not contain preservatives; therefore, discard any unused product. Do not reuse.
- If a dose is missed, administer the dose as soon as possible. Thereafter, resume dosing every 4 weeks.
3 DOSAGE FORMS AND STRENGTHS
OMVOH is a clear to opalescent, colorless to slightly yellow to slightly brown solution available as:
- Intravenous Infusion:
Injection: 300 mg/15 mL (20 mg/mL) solution in a single-dose vial - Subcutaneous Use:
Injection: 100 mg/mL solution in a single-dose prefilled pen
Injection: 100 mg/mL solution in a single-dose prefilled syringe
Injection: 200 mg/2 mL solution in a single-dose prefilled pen
Injection: 200 mg/2 mL (100 mg/mL) solution in a single-dose prefilled syringe
Intravenous Infusion (3)
- Injection: 300 mg/15 mL (20 mg/mL) solution in a single-dose vial
Subcutaneous Injection (3):
- Injection: 100 mg/mL solution in a single-dose prefilled pen
- Injection: 100 mg/mL solution in a single-dose prefilled syringe
- Injection: 200 mg/2 mL solution in a single-dose prefilled pen
- Injection: 200 mg/2 mL (100 mg/mL) solution in a single-dose prefilled syringe
5 WARNINGS AND PRECAUTIONS
- Hypersensitivity Reactions: Serious hypersensitivity reactions, including anaphylaxis and infusion-related reactions, have been reported. If a severe hypersensitivity reaction occurs, discontinue and initiate appropriate treatment. (5.1)
- Infections: OMVOH may increase the risk of infection. Do not initiate treatment with OMVOH in patients with a clinically important active infection until the infection resolves or is adequately treated. If a serious infection develops, do not administer OMVOH until the infection resolves. (5.2)
- Tuberculosis: Do not administer OMVOH to patients with active TB infection. Monitor patients receiving OMVOH for signs and symptoms of active TB during and after treatment. (5.3)
- Hepatotoxicity: Drug-induced liver injury has been reported. Monitor liver enzymes and bilirubin levels at baseline and for at least 24 weeks of treatment and thereafter according to routine patient management. Interrupt treatment if drug-induced liver injury is suspected, until this diagnosis is excluded. (5.4)
- Immunizations: Avoid use of live vaccines. (5.5)
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis during intravenous infusion, have been reported with OMVOH administration. Infusion-related hypersensitivity reactions, including mucocutaneous erythema and pruritus, were reported during induction [see Adverse Reactions (6.1)]. If a severe hypersensitivity reaction occurs, discontinue OMVOH immediately and initiate appropriate treatment.
5.2 Infections
OMVOH may increase the risk of infection [see Adverse Reactions (6.1)].
Do not initiate treatment with OMVOH in patients with a clinically important active infection until the infection resolves or is adequately treated.
In patients with a chronic infection or a history of recurrent infection, consider the risks and benefits prior to prescribing OMVOH. Instruct patients to seek medical advice if signs or symptoms of clinically important acute or chronic infection occur. If a serious infection develops or an infection is not responding to standard therapy, monitor the patient closely and do not administer OMVOH until the infection resolves.
5.3 Tuberculosis
Evaluate patients for tuberculosis (TB) infection prior to initiating treatment with OMVOH.
Do not administer OMVOH to patients with active TB infection. Initiate treatment of latent TB prior to administering OMVOH. Consider anti-TB therapy prior to initiation of OMVOH in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed. Monitor patients for signs and symptoms of active TB during and after OMVOH treatment.
In clinical trials, subjects were excluded if they had evidence of active TB, a past history of active TB, or were diagnosed with latent TB at screening.
5.4 Hepatotoxicity
A case of drug-induced liver injury (alanine aminotransferase [ALT] 18x the upper limit of normal (ULN), aspartate aminotransferase [AST] 10x ULN, and total bilirubin 2.4x ULN) in conjunction with pruritus was reported in a clinical trial subject following a longer than recommended induction regimen. OMVOH was discontinued. Liver test abnormalities eventually returned to baseline.
Evaluate liver enzymes and bilirubin at baseline and for at least 24 weeks of treatment. Monitor thereafter according to routine patient management.
Consider other treatment options in patients with evidence of liver cirrhosis. Prompt investigation of the cause of liver enzyme elevation is recommended to identify potential cases of drug-induced liver injury. Interrupt treatment if drug-induced liver injury is suspected, until this diagnosis is excluded. Instruct patients to seek immediate medical attention if they experience symptoms suggestive of hepatic dysfunction.
5.5 Immunizations
Avoid use of live vaccines in patients treated with OMVOH. Medications that interact with the immune system may increase the risk of infection following administration of live vaccines. Prior to initiating therapy with OMVOH, complete all age-appropriate vaccinations according to current immunization guidelines. No data are available on the response to live or non-live vaccines in patients treated with OMVOH.
6 ADVERSE REACTIONS
The following topics are also discussed in detail in the Warnings and Precautions section:
Most common adverse reactions are:
- Ulcerative colitis (≥2%):
- Crohn's disease (≥5%): upper respiratory tract infections, injection site reactions, headache, arthralgia, and elevated liver tests (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Eli Lilly and Company at 1-800-LillyRx (1-800-545-5979) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Ulcerative Colitis
OMVOH was studied up to 12 weeks in subjects with moderately to severely active ulcerative colitis in a randomized, double-blind, placebo-controlled induction study (UC-1). In subjects who responded to induction therapy in UC-1, long term safety up to 52 weeks was evaluated in a randomized, double-blind, placebo-controlled maintenance study (UC-2) and a long-term extension study [see Clinical Studies (14.1)].
In the induction study (UC-1), 1279 subjects were enrolled of whom 958 received OMVOH 300 mg administered as an intravenous infusion at Weeks 0, 4, and 8. In the maintenance study (UC-2), 581 subjects were enrolled of whom 389 received OMVOH 200 mg administered as a subcutaneous injection every 4 weeks.
Table 2 summarizes the adverse reactions reported in at least 2% of subjects and at a higher frequency than placebo during UC-1.
In the induction study (UC-1), infusion-related hypersensitivity reactions were reported by 4 (0.4%) subjects treated with OMVOH and 1 (0.3%) subject treated with placebo.
Table 3 summarizes the adverse reactions reported in at least 2% of subjects and at a higher frequency than placebo during the 40-week controlled period of UC-2.
Infections
In UC-1 through Week 12, infections were reported by 145 (15%) subjects treated with OMVOH 300 mg and 45 (14%) subjects treated with placebo. Serious infections were reported by less than 1% in both groups. Serious infections in the OMVOH group included intestinal sepsis, listeria sepsis, and pneumonia.
In the maintenance study (UC-2) through Week 40 (a total of 52 weeks of treatment), infections were reported by 93 (24%) subjects treated with OMVOH 200 mg and 44 (23%) subjects treated with placebo. A case of COVID-19 pneumonia was reported as a serious infection in the OMVOH group.
Hepatic Enzyme Elevations
In UC-1 through Week 12, alanine aminotransferase (ALT) ≥5X ULN was reported by 1 (0.1%) subject treated with OMVOH 300 mg and 1 (0.3%) subject treated with placebo. Aspartate aminotransferase (AST) ≥5X ULN was reported by 2 (0.2%) subjects treated with OMVOH 300 mg and no subject treated with placebo. These elevations have been noted with and without concomitant elevations in total bilirubin.
In UC-2 through Week 40 (a total of 52 weeks of treatment), 3 (0.8%) subjects treated with OMVOH 200 mg reported ALT ≥5X ULN and 3 (0.8%) subjects reported AST ≥5X ULN; with or without concomitant elevations in total bilirubin. No subjects treated with placebo experienced similar elevations [see Warnings and Precautions (5.4)].
Crohn's Disease
OMVOH was studied up to 52 weeks in subjects with moderately to severely active Crohn's disease in a randomized, double-blind, placebo-controlled study (CD-1). The safety population consisted of 630 subjects who received OMVOH 900 mg administered as an intravenous infusion during induction at Weeks 0, 4, and 8 followed by OMVOH 300 mg administered as a subcutaneous injection every 4 weeks and 211 subjects who received placebo [see Clinical Trials (14.2)]. Eighty-five of the 211 placebo subjects in the safety population who did not achieve clinical response by patient-reported outcome at Week 12 were switched to blinded induction and maintenance treatment with OMVOH. Observed data from these 85 subjects are included in the placebo cohort up to Week 12 and in the OMVOH cohort after Week 12. In CD-1, OMVOH and placebo-treated subjects had different lengths of exposure, therefore, exposure adjusted incidence rates (EAIRs) are also displayed in Table 4 to compare adverse reactions.
Common Adverse Reactions
Table 4 summarizes the frequencies and EAIRs per 100 person-years (PY) for adverse reactions reported in at least 5% of subjects treated with OMVOH and at a higher frequency than placebo during CD-1.
Hepatic Enzyme Elevations
Of the subjects with reported adverse reactions of elevated liver tests (see Table 4), 3 subjects treated with OMVOH reported ALT ≥5X ULN and 2 subjects reported AST ≥5X ULN. Neither subject had a concomitant elevation in total bilirubin. No subjects treated with placebo experienced similar elevations.
Less Common Adverse Reactions (<5%)
In CD-1 through Week 52, urticaria was reported by 13 (2%, 2 per 100 PY) subjects treated with OMVOH and no subjects treated with placebo.
Infections
In CD-1 through Week 52, infections were reported by 282 (39%, 58 per 100 PY) subjects treated with OMVOH and 73 (35%, 81 per 100 PY) subjects treated with placebo. Serious infections in the OMVOH group included abscess (including abdominal abscess, anal abscess, gluteal abscess, and perineal abscess), cellulitis, pneumonia, and sepsis.
7 DRUG INTERACTIONS
7.1 CYP450 Substrates
Increased concentrations of cytokines (e.g., IL-1, IL-6, IL-10, TNFα, IFN) during chronic inflammation associated with certain diseases including Crohn's disease may suppress the formation of CYP450 enzymes. Therapeutic proteins, including mirikizumab-mrkz, that decrease the concentrations of these pro-inflammatory cytokines may increase the formation of CYP450 enzymes resulting in decreased CYP450 substrate exposure. Upon initiation or discontinuation of OMVOH in patients treated with concomitant CYP450 substrates, monitor drug concentrations or other therapeutic parameters, and adjust the dosage of the CYP450 substrate as needed. See the prescribing information of specific CYP450 substrates.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There will be a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to OMVOH during pregnancy. Pregnant women exposed to OMVOH and healthcare providers are encouraged to call Eli Lilly and Company at 1-800-Lilly-Rx (1-800-545-5979).
Risk Summary
Available data from case reports of mirikizumab-mrkz use in pregnant women are insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Although there are no data on mirikizumab-mrkz, monoclonal antibodies can be actively transported across the placenta, and mirikizumab-mrkz may cause immunosuppression in the in utero-exposed infant. An enhanced pre- and post-natal development study conducted in pregnant monkeys at a dose 20 times the maximum recommended human dose (MRHD) revealed no adverse developmental effects to the developing fetus, or harm to infant monkeys from birth through 6 months of age. There are risks of adverse pregnancy outcomes associated with increased disease activity in women with inflammatory bowel disease (see Clinical Considerations).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defects, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and Embryo/Fetal Risk
Published data suggest that the risk of adverse pregnancy outcomes in women with inflammatory bowel disease (IBD) is associated with increased disease activity. Adverse pregnancy outcomes include preterm delivery (before 37 weeks gestation), low birth weight (less than 2500 g) infants, and small for gestational age at birth.
Fetal/Neonatal Adverse Reactions
Transport of endogenous IgG antibodies across the placenta increases as pregnancy progresses, and peaks during the third trimester. It is unclear whether mirikizumab-mrkz may interfere with an infant's immune response to infections. Therefore, monitoring for the development of serious infection during the first 2 months of life in infants exposed in utero is recommended.
Data
Animal Data
An enhanced pre- and postnatal development study was conducted in cynomolgus monkeys administered mirikizumab-mrkz by intravenous injection during organogenesis to parturition at a dose of 300 mg/kg twice weekly (20 times the MRHD based on exposure comparisons). Mirikizumab-mrkz crossed the placenta in monkeys. No maternal toxicity was noted in this study. No mirikizumab-mrkz-related effects on morphological, functional or immunological development were observed in infant monkeys from birth through 6 months of age. However, incidences of embryo/fetal loss were higher in the treated groups compared to control (6.7% [1 of 15] in controls vs 26.7% [4 of 15] at 300 mg/kg (20 times the MRHD, based on exposure comparisons) but were within the range of historical control data. Following delivery, most adult female cynomolgus monkeys and all infants from the mirikizumab-mrkz-treated group had measurable serum concentrations up to 28 days postpartum. In the infant monkeys, mean serum concentrations were approximately 4.8 times the respective mean maternal concentrations.
8.2 Lactation
Risk Summary
There are no data on the presence of mirikizumab-mrkz in human milk, the effects on the breastfed infant, or the effects on milk production. Endogenous maternal IgG and monoclonal antibodies are transferred in human milk. The effects of local gastrointestinal exposure and limited systemic exposure in the breastfed infant to mirikizumab-mrkz are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for OMVOH and any potential adverse effects on the breastfed infant from OMVOH or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of OMVOH have not been established in pediatric patients.
8.5 Geriatric Use
Of the 795 OMVOH-treated subjects in the two ulcerative colitis clinical studies, 64 subjects (8%) were 65 years of age and older, while 10 subjects (1%) were 75 years of age and older. Of the 715 OMVOH-treated subjects in the Crohn's disease clinical study, 22 subjects (3%) were 65 years of age and older, while 6 subjects (1%) were 75 years of age and older). These clinical studies did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger adult subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger subjects. No clinically meaningful differences in the pharmacokinetics of mirikizumab-mrkz were observed in subjects 65 years of age and older compared to younger adult subjects [see Clinical Pharmacology (12.3)].
11 DESCRIPTION
Mirikizumab-mrkz is a humanized immunoglobulin G4 (IgG4) variant monoclonal antibody that is directed against the p19 subunit of IL-23 and does not bind IL-12. Mirikizumab-mrkz is produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology and it is composed of two identical light chain polypeptides and two identical heavy chain polypeptides with an overall molecular weight of approximately 147 kDa.
OMVOH for intravenous infusion for ulcerative colitis and Crohn's disease
OMVOH (mirikizumab-mrkz) injection is a sterile, preservative-free, clear to opalescent, colorless to slightly yellow to slightly brown solution in a single-dose vial for intravenous infusion after dilution.
OMVOH injection 300 mg /15 mL vial is available in 2 formulations:
- Each mL contains 20 mg of mirikizumab-mrkz, anhydrous citric acid (0.4 mg), polysorbate 80 (0.5 mg), sodium chloride (8.8 mg), sodium citrate (2.1 mg), and Water for Injection. The OMVOH solution has a pH range of 5.0 to 6.0.
- Each mL contains 20 mg of mirikizumab-mrkz, anhydrous citric acid (0.1 mg), histidine (0.1 mg), L-histidine hydrochloride monohydrate (0.9 mg), mannitol (33 mg), polysorbate 80 (0.5 mg), sodium chloride (2.9 mg), sodium citrate (0.2 mg), and Water for Injection. The OMVOH solution has a pH range of 5.0 to 5.8.
OMVOH (mirikizumab-mrkz) injection 100 mg/mL prefilled pen or prefilled syringe for subcutaneous use for ulcerative colitis and Crohn's disease
OMVOH (mirikizumab-mrkz) injection is a sterile, preservative free, clear to opalescent, colorless to slightly yellow to slightly brown solution for subcutaneous use available as 100 mg of mirikizumab-mrkz in a 1 mL single-dose prefilled pen or single-dose prefilled syringe. The prefilled pen and prefilled syringe contain a 1 mL glass syringe with a fixed 27-gauge ½ inch needle. The OMVOH 100 mg prefilled pen and prefilled syringe are manufactured to deliver 100 mg of mirikizumab-mrkz.
Each mL is composed of 100 mg mirikizumab-mrkz, histidine (0.1 mg), L-histidine hydrochloride monohydrate (0.9 mg), mannitol (33 mg), polysorbate 80 (0.3 mg), sodium chloride (2.9 mg), and Water for Injection. The OMVOH solution has a pH range of 5.0 to 5.8.
OMVOH (mirikizumab-mrkz) injection 200 mg/2 mL prefilled pen or 200 mg/2 mL (100 mg/mL) prefilled syringe for subcutaneous use for ulcerative colitis and Crohn's disease
OMVOH (mirikizumab-mrkz) injection is a sterile, preservative free, clear to opalescent, colorless to slightly yellow to slightly brown solution for subcutaneous use. The 2 mL prefilled pen and prefilled syringe each contain a 2 mL glass syringe with a fixed 27-gauge 8 mm needle. The OMVOH 200 mg prefilled pen and prefilled syringe are manufactured to deliver 200 mg of mirikizumab-mrkz.
Each mL is composed of 100 mg mirikizumab-mrkz, histidine (0.1 mg), L-histidine hydrochloride monohydrate (0.9 mg), mannitol (33 mg), polysorbate 80 (0.3 mg), sodium chloride (2.9 mg), and Water for Injection. The OMVOH solution has a pH range of 5.0 to 5.8.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Mirikizumab-mrkz is a humanized IgG4 monoclonal antibody that selectively binds to the p19 subunit of human IL-23 cytokine and inhibits its interaction with the IL-23 receptor.
IL-23 is involved in mucosal inflammation and affects the differentiation, expansion, and survival of T cell subsets, and innate immune cell subsets, which represent sources of pro-inflammatory cytokines. Research in animal models has shown that pharmacologic inhibition of IL-23p19 can ameliorate intestinal inflammation.
Mirikizumab-mrkz inhibits the release of pro-inflammatory cytokines and chemokines.
12.2 Pharmacodynamics
In both study UC-1 (induction) and study UC-2 (maintenance), a positive relationship was observed between Mirikizumab-mrkz average concentration and rates of clinical remission and clinical response [see Clinical Studies (14.1)].
Mirikizumab exposure response relationships have not been fully characterized in subjects with Crohn's disease.
12.3 Pharmacokinetics
Mirikizumab-mrkz exhibited linear pharmacokinetics with dose-proportional increase in exposure over a dose range of 60 to 2400 mg given as an intravenous injection or over a dose range of 200 to 400 mg given as a subcutaneous injection, in healthy volunteers. There was no apparent accumulation of mirikizumab-mrkz concentrations in serum over time when administered as a subcutaneous injection every 4 weeks to subjects with ulcerative colitis or Crohn's disease. The estimated exposure parameters of mirikizumab-mrkz at steady state are summarized in Tables 5 for ulcerative colitis and 6 for Crohn's disease.
Absorption
Following subcutaneous dosing of OMVOH for ulcerative colitis median (range) Tmax was 5 (3.08 to 6.75) days post dose and geometric mean (CV%) absolute bioavailability was 44% (34%).
Following subcutaneous dosing of OMVOH for Crohn's disease, median (range) Tmax was 5 (3 to 6.83) days post dose and geometric mean (CV%) absolute bioavailability was 36.3% (31%).
Injection site location (abdomen, upper arm, or thigh) did not significantly influence bioavailability of mirikizumab-mrkz following subcutaneous injection.
Distribution
In subjects with ulcerative colitis, the geometric mean (CV%) total volume of distribution was 4.83 L (21%).
In subjects with Crohn's disease, the geometric mean (CV%) total volume of distribution was 4.4 L (14%).
Metabolism/Elimination
Mirikizumab-mrkz is a humanized IgG4 monoclonal antibody and is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG.
In subjects with ulcerative colitis, the geometric mean (CV%) clearance was 0.0229 L/hours (34%) and the geometric mean (CV%) elimination half-life was 9.3 days (40%). Clearance is independent of dose.
In subjects with Crohn's disease, the geometric mean (CV%) clearance was 0.0202 L/hours (38%) and the geometric mean (CV%) elimination half-life was 9.3 days (26%). Clearance is independent of dose.
Specific Populations
There were no clinically significant differences in the pharmacokinetics of mirikizumab-mrkz based on age (18 to 79 years), sex, race (White or Asian), or mild and moderate renal impairment (i.e., estimated creatinine clearance by Cockcroft-Gault equation: 30 to 89 mL/min).
Body Weight
Following intravenous administration of 300 mg, the recommended induction dose, in subjects with ulcerative colitis weighing 90 kg or greater, the estimated geometric mean mirikizumab-mrkz average concentration (Cavg) was 20% lower compared with subjects weighing less than 90 kg. Following subcutaneous administration of 200 mg, the recommended maintenance dose, in subjects with ulcerative colitis weighing 90 kg or greater, the estimated geometric mean Cavg was 38% lower compared with subjects weighing less than 90 kg. In Study UC-2 (maintenance), the rate of clinical remission and clinical response did not differ significantly between subjects weighing 90 kg or greater and subjects weighing less than 90 kg.
Following intravenous administration of 900 mg, the recommended induction dose, in subjects with Crohn's disease weighing 90 kg or greater, the estimated geometric mean mirikizumab-mrkz Cavg was 13% lower compared with subjects weighing less than 90 kg. Following subcutaneous administration of 300 mg, the recommended maintenance dose, in subjects with Crohn's disease weighing 90 kg or greater, the estimated geometric mean Cavg was 34% lower compared with subjects weighing less than 90 kg. The rate of clinical remission and clinical response in Crohn's disease did not differ significantly between subjects weighing 90 kg or greater and subjects weighing less than 90 kg.
Drug Interaction Studies
Population pharmacokinetic analyses indicated that the clearance of OMVOH was not impacted by concomitant administration of aminosalicylates, corticosteroids, or oral immunomodulators (6-MP, AZA, MTX, tioguanine) in subjects with ulcerative colitis or Crohn's disease.
No drug-drug interaction studies were conducted in subjects with ulcerative colitis or Crohn's disease at the recommended dosage. Based on a clinical drug-drug interaction study conducted in subjects with another condition, multiple subcutaneous doses of 250 mg every 4 weeks of mirikizumab-mrkz did not result in changes in the exposure of midazolam (CYP3A substrate), warfarin (CYP2C9 substrate), dextromethorphan (CYP2D6 substrate), omeprazole (CYP2C19 substrate), or caffeine (CYP1A2 substrate).
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies, including those of mirikizumab-mrkz or of other mirikizumab products.
During the 52-week treatment period in studies UC-1 and UC-2, 23% (88/378) of OMVOH-treated subjects at the recommended dosage and evaluable for assessment, developed anti-mirikizumab-mrkz antibodies (referred to as anti-drug antibodies (ADA)). Of those who developed ADA, 33/88 (38%) developed titers ≥1:160. Of these 33 OMVOH-treated subjects, 10 had reduced serum trough concentrations of mirikizumab-mrkz compared to subjects who did not develop anti-mirikizumab-mrkz antibodies, and 5 of these 10 subjects did not achieve clinical response at Week 52. There is insufficient data to assess whether the observed ADA-associated pharmacokinetic changes reduced effectiveness. There is no identified clinically significant effect of ADA on the safety of OMVOH over the treatment duration of 52-weeks.
During the 52-week treatment period in study CD-1, 13% (79/622) of OMVOH-treated subjects at the recommended dosage and evaluable for assessment developed ADA. There is no identified clinically significant effect of ADA on the pharmacokinetics, effectiveness, or safety of OMVOH over the treatment duration of 52-weeks.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Animal studies have not been conducted to evaluate the carcinogenic or mutagenic potential of mirikizumab-mrkz.
No organ weight or histopathology effects were observed in the male or female reproductive tract in sexually mature cynomolgus monkeys that received subcutaneous mirikizumab-mrkz once weekly for 26 weeks, at a dose of 100 mg/kg (at least 2 times the MRHD of mirikizumab-mrkz, based on exposure comparisons).
14 CLINICAL STUDIES
14.1 Ulcerative Colitis
The safety and efficacy of OMVOH was evaluated in two randomized, double-blind, placebo-controlled clinical studies, one induction study [UC-1 (NCT03518086)] and one maintenance study [UC-2 (NCT03524092)], in adult subjects with moderately to severely active ulcerative colitis who had inadequate response, loss of response, or failed to tolerate any of the following: corticosteroids, 6-mercaptopurine, azathioprine, biologic therapy (TNF blocker, vedolizumab), or tofacitinib. The 12-week intravenous induction study (UC-1) was followed by the 40-week subcutaneous randomized withdrawal maintenance study (UC-2).
Study UC-1
In UC-1, efficacy was evaluated in 1062 subjects who were randomized 3:1 at Week 0 to receive 300 mg OMVOH or placebo by intravenous infusion at Week 0, Week 4, and Week 8. Subjects had a mean age of 43 years (range 18 to 79 years); 40% were female; and 71% identified as White, 25% as Asian, 1% as American Indian or Alaska Native, 1% as Black or African American, and <2% as another racial group or did not report their racial group. Subjects were permitted to use stable doses of aminosalicylates, immunomodulators (6-mercaptopurine, azathioprine, methotrexate), and oral corticosteroids (prednisone ≤20 mg/day or equivalent, extended-release budesonide 9 mg/day, beclomethasone dipropionate 5 mg/day). At baseline, 41% of subjects were receiving oral corticosteroids, 24% were receiving immunomodulators, and 75% were receiving aminosalicylates.
At baseline, 57% were biologic and Janus Kinase inhibitor (JAKi) naive, 41% had failed at least one biologic, 3% had failed a JAKi, and 2% had previously received but had not failed a biologic or JAKi.
Disease activity was assessed based on the modified Mayo score (mMS), which ranges from 0 to 9 and has three subscores that are each scored from 0 (normal) to 3 (most severe): stool frequency, rectal bleeding, and findings on centrally read endoscopy subscore. At baseline, subjects had a mMS of 5 to 9, including a centrally read endoscopy subscore of 2 or 3. An endoscopy subscore of 2 was defined by marked erythema, absent vascular pattern, friability, and erosions; and a subscore of 3 was defined by spontaneous bleeding and ulceration. Subjects had a median mMS of 7, and 58% had severely active disease (mMS of 7 to 9).
The primary endpoint was clinical remission at Week 12. The secondary endpoints were clinical response, endoscopic improvement, and histologic-endoscopic mucosal improvement (see Table 7).
Study UC-1 was not designed to evaluate the relationship of histologic-endoscopic mucosal improvement at Week 12 to disease progression and long-term outcomes.
Rectal Bleeding and Stool Frequency Subscores
Decreases in rectal bleeding and stool frequency subscores were observed as early as Week 3 in subjects treated with OMVOH compared to subjects on placebo.
Study UC-2
The maintenance study (UC-2) evaluated 506 subjects who achieved clinical response at Week 12 in Study UC-1. These subjects were randomized 2:1 to receive 200 mg OMVOH or placebo subcutaneously every 4 weeks for 40 weeks in UC-2, for a total of 52 weeks of treatment. Subjects who were on concomitant ulcerative colitis therapies during UC-1 were required to continue on stable doses of oral aminosalicylates and immunomodulators (6-mercaptopurine, azathioprine, methotrexate). Corticosteroid tapering was required for subjects who were receiving corticosteroids at baseline and achieved clinical response in UC-1.
The primary endpoint was clinical remission at Week 40. The secondary endpoints were endoscopic improvement, maintenance of clinical remission in subjects who achieved clinical remission at Week 12, corticosteroid-free clinical remission, and histologic-endoscopic mucosal improvement (see Table 8).
Study UC-2 was not designed to evaluate the relationship of histologic-endoscopic mucosal improvement at Week 40 to disease progression and long-term outcomes.
Bowel Urgency
Bowel urgency was assessed during UC-1 and UC-2 with an Urgency Numeric Rating Scale (NRS) of 0 to 10. A greater proportion of subjects with a baseline Urgency NRS weekly average score ≥3 treated with OMVOH compared to placebo reported an Urgency NRS weekly average score of 0 or 1 (39% versus 23%) at Week 40. Urgency NRS weekly average scores of 0 to 1 were also observed in a greater proportion of subjects treated with OMVOH compared to placebo at Week 12.
Endoscopic Assessment
Normalization of the endoscopic appearance of the mucosa (endoscopic remission) was defined as a Mayo endoscopic subscore of 0. At Week 40 in UC-2, endoscopic remission was observed in a greater proportion of subjects treated with OMVOH compared to placebo (22% versus 14%).
14.2 Crohn's Disease
The safety and efficacy of OMVOH was evaluated in a randomized, double-blind, placebo-controlled study [CD-1 (NCT03926130)] in adult subjects with moderately to severely active Crohn's disease who had an inadequate response, loss of response, or intolerance to corticosteroids, immunomodulators (azathioprine, 6-mercaptopurine, and methotrexate), and/or biologics (TNF blockers, integrin receptor antagonists).
In CD-1, the efficacy population consisted of 679 subjects who were randomized 3:1 at Week 0 to receive OMVOH 900 mg by intravenous infusion at Week 0, Week 4, and Week 8 followed by a dosage of 300 mg by subcutaneous injection at Week 12 and then every 4 weeks for 40 weeks, or placebo. Subjects had a mean age of 36 years (range 18 to 74 years); 42% were female; and 71% identified as White, 25% as Asian, <1% as American Indian or Alaska Native, 1% as Black or African American, and 2% as another racial group or did not report their racial group. Subjects were permitted to use stable doses of oral corticosteroids (prednisone ≤30 mg/day or equivalent, extended-release budesonide 9 mg/day), immunomodulators (6-mercatopurine, azathioprine, or methotrexate) and/or aminosalicylates. At baseline, 31% of subjects were receiving oral corticosteroids, 26% were receiving immunomodulators, and 44% were receiving aminosalicylates.
At baseline, 47% had a loss of response, inadequate response, or intolerance to one or more biologic therapy.
Disease activity at baseline was assessed by the Crohn's Disease Activity Index (CDAI) and the Simple Endoscopic Score for Crohn's disease (SES-CD). Moderately to severely active CD was defined by a CDAI of ≥220 and an SES-CD ≥7 (centrally read) for subjects with ileal-colonic disease or ≥4 for subjects with isolated ileal disease. At baseline, subjects had a median CDAI of 329 and SES-CD of 12.
The coprimary endpoints of clinical remission by CDAI and endoscopic response by SES-CD were assessed at Week 52. Secondary efficacy endpoints included endoscopic response at Week 12 and endoscopic remission and corticosteroid-free clinical remission at Week 52 (see Table 9).
Stool Frequency and Abdominal Pain
In CD-1, reductions in abdominal pain were observed as early as Week 6 and in stool frequency as early as Week 12 in subjects treated with OMVOH compared to placebo.
Fatigue
In CD-1, subjects treated with OMVOH experienced a clinically meaningful improvement in fatigue, assessed by the change from baseline in the Functional Assessment of Chronic Illness Therapy Fatigue Scale (FACIT-Fatigue), at Week 12, compared to placebo-treated subjects. The effect of OMVOH to improve fatigue after 12 weeks has not been established.
Other Assessments at Week 12
In CD-1, a greater proportion of subjects treated with OMVOH compared to placebo achieved clinical remission (34% versus 23%) and endoscopic remission (10% versus 4%) at Week 12.
16 HOW SUPPLIED/STORAGE AND HANDLING
OMVOH (mirikizumab-mrkz) injection is a sterile, preservative-free, clear to opalescent, colorless to slightly yellow to slightly brown solution for intravenous infusion or subcutaneous injection.
OMVOH is supplied in indication specific packaging as:
Note to Pharmacist: The entire carton of 2 prefilled pen or 2 prefilled syringes are to be dispensed as a unit.
Each 100 mg/mL single-dose prefilled pen or prefilled syringe consists of a 1 mL glass syringe with a fixed 27-gauge ½ inch needle.
Each 200 mg/2 mL single-dose prefilled pen or 200 mg/2 mL (100 mg/mL) prefilled syringe consists of a 2 mL glass syringe with a fixed 27-gauge 8 mm needle.
Storage and Handling
- Store refrigerated at 2°C to 8°C (36°F to 46°F).
- Do not freeze. Do not use OMVOH if it has been frozen.
- Do not shake.
- Keep OMVOH in the original carton to protect from light until the time of use.
- OMVOH is sterile and preservative-free. Discard any unused portion.
- If needed, the prefilled pen or prefilled syringe may be stored at room temperature up to 30°C (86°F) for up to 2 weeks in the original carton to protect from light. Once OMVOH has been stored at room temperature, do not return to the refrigerator. If these conditions are exceeded, OMVOH must be discarded.
- The vial, prefilled pen, and prefilled syringe are not made with dry natural rubber latex.
17 PATIENT COUNSELING INFORMATION
Advise the patient and/or caregiver to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Hypersensitivity Reactions
Advise patients to discontinue OMVOH and seek immediate medical attention if they experience any symptoms of serious hypersensitivity reactions [see Warnings and Precautions (5.1)].
Infections
Advise patients that OMVOH may lower the ability of their immune system to fight infections and to contact their healthcare provider immediately if they develop any symptoms of infection [see Warnings and Precautions (5.2)].
Tuberculosis
Advise patients to contact their healthcare provider if they experience symptoms suggestive of TB (e.g., unexplained fever, cough, or difficulty breathing) [see Warnings and Precautions (5.3)].
Hepatotoxicity
Inform patients that OMVOH may cause liver injury. Advise patients to seek immediate medical attention if they experience symptoms suggestive of liver dysfunction (e.g., unexplained rash, nausea, vomiting, abdominal pain, fatigue, anorexia, or jaundice and/or dark urine) [see Warnings and Precautions (5.4)].
Immunizations
Advise patients that vaccination with live vaccines is not recommended during OMVOH treatment and immediately prior to or after OMVOH treatment. Medications that interact with the immune system may increase the risk of infection following administration of live vaccines. Instruct patients to inform their healthcare provider that they are taking OMVOH prior to receiving a vaccination [see Warnings and Precautions (5.5)].
Pregnancy
Advise patients who are exposed to OMVOH during pregnancy to contact Eli Lilly and Company [see Use in Specific Populations (8.1)].
Administration
Instruct patients in preparation and administration of OMVOH, including choosing anatomical sites for subcutaneous administration, and proper subcutaneous injection technique. Instruct patients in the technique of prefilled pen or prefilled syringe disposal [see Instructions for Use].
Instruct ulcerative colitis patients or caregivers to administer either:
- Two 100 mg prefilled pens or two 100 mg prefilled syringes to achieve the full 200 mg dose of OMVOH.
- One 200 mg prefilled pen or one 200 mg prefilled syringe to achieve the full 200 mg dose of OMVOH.
Instruct Crohn's disease patients or caregivers to administer a 100 mg prefilled pen or prefilled syringe and a 200 mg prefilled pen or prefilled syringe in any order to achieve the full 300 mg dose of OMVOH.
Eli Lilly and Company, Indianapolis, IN 46285, USA
US License No. 1891
Copyright © 2023, 2025, Eli Lilly and Company. All rights reserved.
Pat.: www.lilly.com/patents
OMV-0009-USPI-20251104
OMV-0005-MG-20251027
100 MG PREFILLED PEN INSTRUCTIONS FOR USE













This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOH™ is a trademark of Eli Lilly and Company.
Copyright © 2023, 2025, Eli Lilly and Company. All rights reserved.
Revised: October 2025
The OMVOH prefilled Pen meets the current dose accuracy and functional requirements of ISO 11608-1 and 11608-5.
OMV-0005-IFU-PEN-20251023
100 MG PREFILLED SYRINGE INSTRUCTIONS FOR USE







This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOHTM is a trademark of Eli Lilly and Company.
Copyright © 2024, 2025, Eli Lilly and Company. All rights reserved.
Revised: October 2025
OMV-0003-IFU-PFS-20251023
100 MG + 200 MG PREFILLED PEN INSTRUCTIONS FOR USE
INSTRUCTIONS FOR USE
OMVOH TM (ahm-voh)
(mirikizumab-mrkz)
injection, for subcutaneous use
Prefilled Pens
One 200 mg/2 mL Prefilled Pen and one 100 mg/mL Prefilled Pen for a full dose of 300 mg

This Instructions for Use contains information on how to inject OMVOH.
Before you use the OMVOH prefilled Pens, read and carefully follow all the step-by-step instructions.
Important information you need to know before injecting OMVOH
- Your healthcare provider should show you how to prepare and inject OMVOH using the prefilled Pens. Do not inject yourself or someone else until you have been shown how to inject OMVOH.
- Keep this Instructions for Use and read it as needed.
- Each OMVOH prefilled Pen is for one-time use only.
- The OMVOH prefilled Pen contains glass parts. Handle it carefully. If you drop it on a hard surface, do not use it. Use a new OMVOH prefilled Pen for your injection.
- Your healthcare provider can help you decide where on your body to inject your dose. Read the Choose and clean your injection sites section of these instructions to help you choose which area can work best for you.
- If you have vision or hearing problems, do not use OMVOH prefilled Pens without help from a caregiver.
- See Storing OMVOH Prefilled Pens for important storage information.
INSTRUCTIONS FOR USE
Before you use the OMVOH prefilled Pens, read and carefully follow all the step-by-step instructions.
2 Prefilled Pens = full 300 mg dose
After your first injection, choose a new injection site at least 2 inches (5 centimeters) away and clean it.
With your second prefilled Pen, repeat steps 1 to 3 right away after your first injection.
You must inject 2 prefilled Pens to complete your full 300 mg dose.
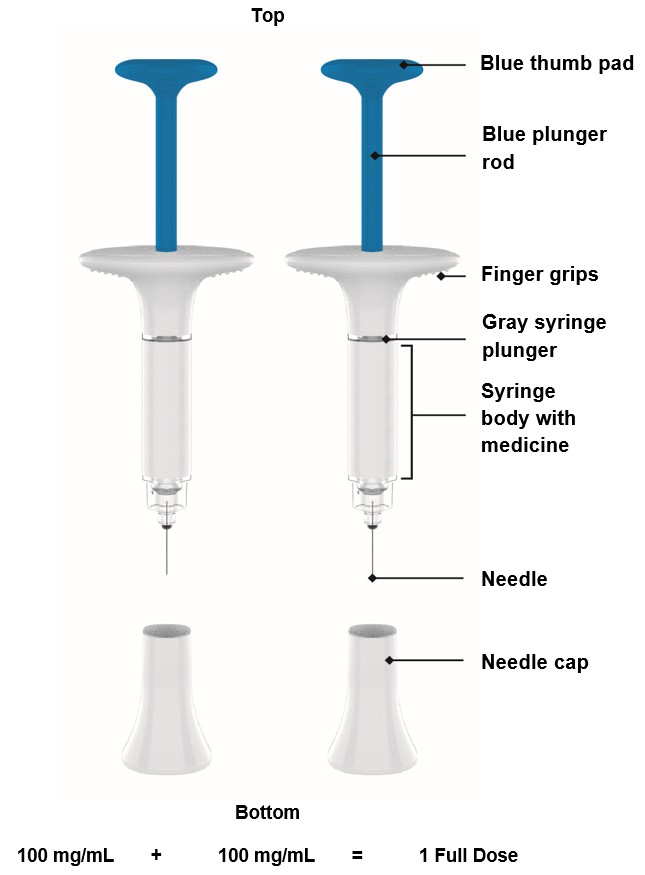
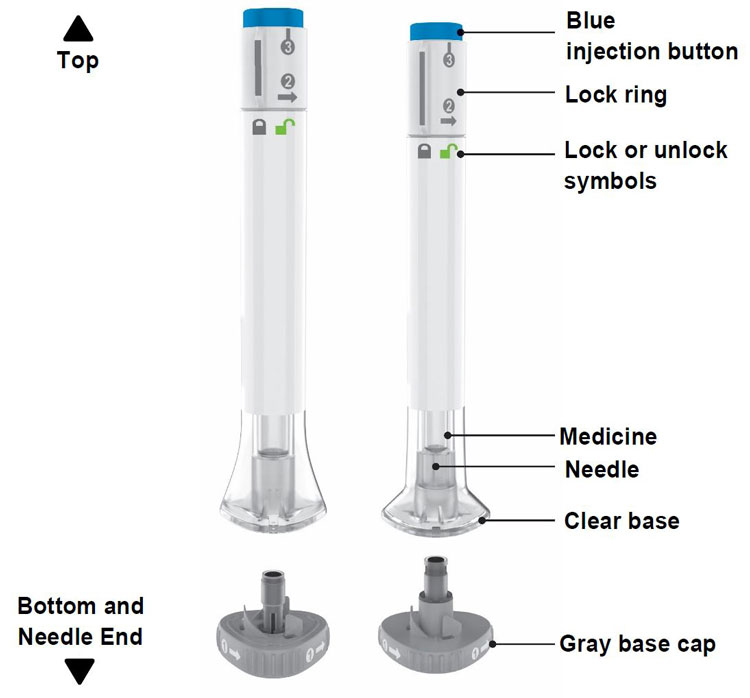
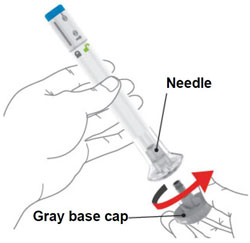
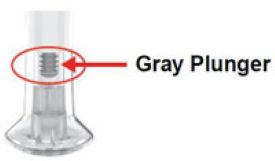
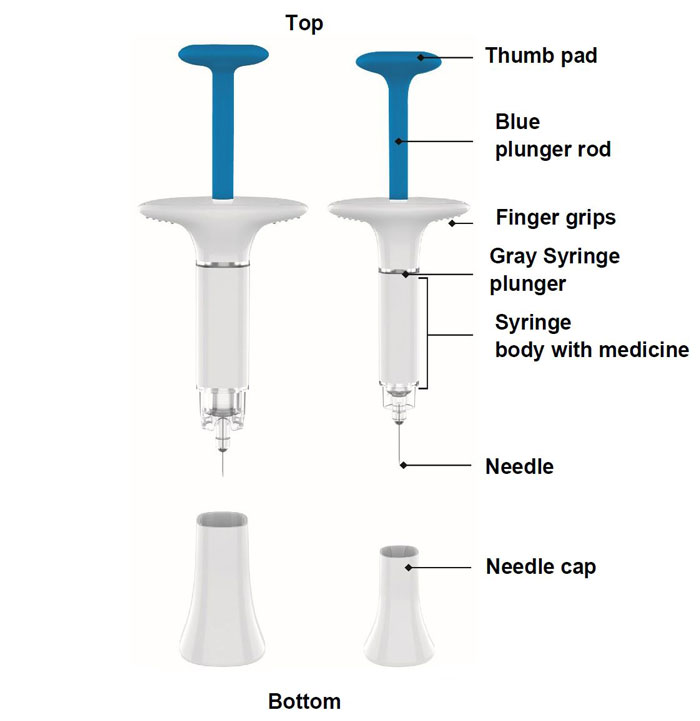
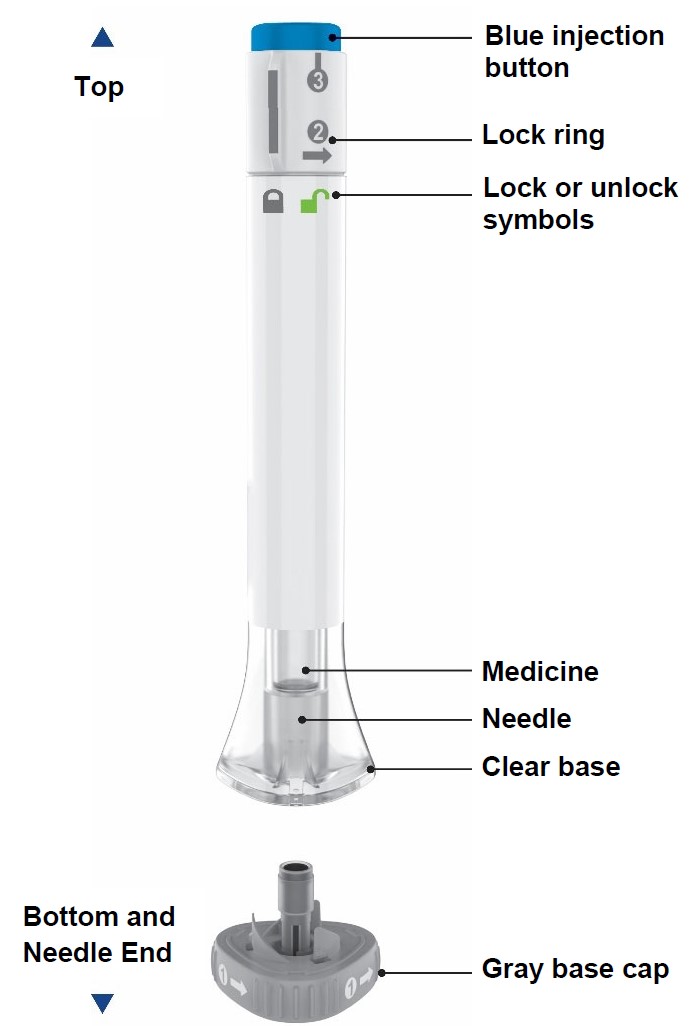
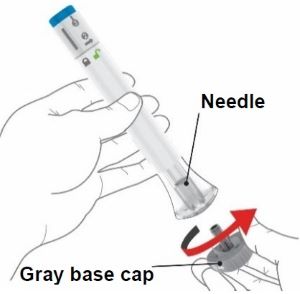
Parts of the OMVOH Prefilled Pens
Inject both prefilled Pens in any order for a full 300 mg dose.
The 200 mg/2 mL prefilled Pen is larger than the 100 mg/mL prefilled Pen.
Preparing to inject OMVOH
Gather supplies
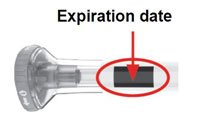
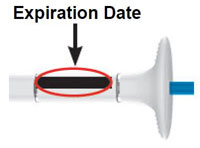
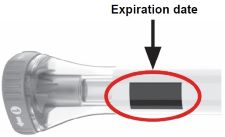
Inspect the prefilled Pens and the medicine
Remove both prefilled Pens from the carton.
Make sure you have the right medicine.
The medicine inside should be clear. It may be colorless to slightly yellow to slightly brown.
Wait 45 minutes
Do not warm up the prefilled Pens with a microwave, hot water, or direct sunlight.
With the gray base cap on, allow the prefilled Pens to warm up to room temperature for 45 minutes before injecting.
Choose and clean your injection sites
Your healthcare provider can help you choose the injection sites that are best for you. Clean the injection sites with an alcohol wipe and let them dry.
Injecting OMVOH
1. Uncap the first prefilled Pen (the prefilled Pens may be used in any order)

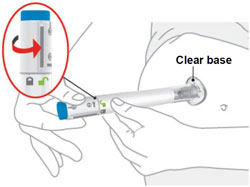
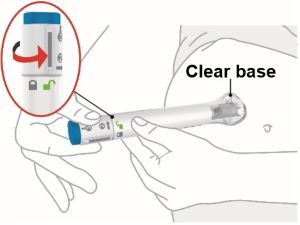
2. Place and unlock
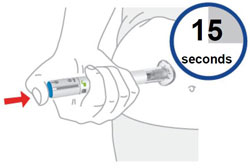
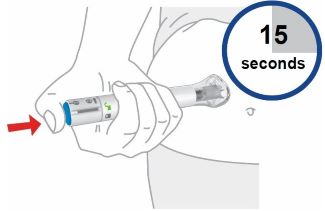
3. Press and hold for 15 seconds
4. Inject the second prefilled Pen
Choose a new injection site at least 2 inches away and clean it.
With your second prefilled Pen, repeat steps 1 to 3 right away after your first injection.
You must inject 2 prefilled Pens to complete your full 300 mg dose.
Throwing away (disposing of) OMVOH Prefilled Pens
Throw away both used prefilled Pens

Storing OMVOH Prefilled Pens
Refrigeration
- In the original carton, store your prefilled pens in the refrigerator between 36°F to 46°F (2°C to 8°C) until the expiration date.
- Do not freeze. Do not use OMVOH if it has been frozen.
Room Temperature
- If needed, your prefilled Pens may be stored at room temperature for up to 2 weeks in the original carton. Do not store above 86°F (30°C).
- When OMVOH has been stored at room temperature, do not return it to the refrigerator.
- Throw away (dispose of) OMVOH if not used within 2 weeks at room temperature.
- Protect your prefilled Pens from light until use.
Do not use the prefilled Pens and throw away (see Throwing away (disposing of) OMVOH Prefilled Pens) if they have been:
Keep OMVOH and all medicines out of the reach of children.
Commonly asked questions
Additional Information:
If you have more questions about how to use the OMVOH prefilled Pens:
Used OMVOH Prefilled Pen disposal
Put the used OMVOH prefilled Pens in an FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) the OMVOH prefilled Pens in your household trash.
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container.
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container.
There may be state or local laws about how you should throw away needles and syringes.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
Do not recycle your used sharps disposal container.
Read the Medication Guide for OMVOH inside this box to learn more about your medicine.
Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOHTM is a trademark of Eli Lilly and Company.
Copyright © 2025, Eli Lilly and Company. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Approved: January 2025
The OMVOH prefilled Pen meets the current dose accuracy and functional requirements of ISO 11608-1 and 11608-5.
OMV-0001-300MG-PEN-IFU-20250115
100 MG + 200 MG PREFILLED SYRINGE INSTRUCTIONS FOR USE
INSTRUCTIONS FOR USE
OMVOH TM (ahm-voh)
(mirikizumab-mrkz)
injection, for subcutaneous use
Prefilled Syringes
One 200 mg/2 mL (100 mg/mL) Prefilled Syringe and One 100 mg/mL Prefilled Syringe for a Full Dose of 300 mg.

This Instructions for Use contains information on how to inject OMVOH.
Before you use the OMVOH prefilled Syringes, read and carefully follow all the step-by-step instructions.
Important information you need to know before injecting OMVOH
- Your healthcare provider should show you how to prepare and inject OMVOH using the prefilled Syringes. Do not inject yourself or someone else until you have been shown how to inject OMVOH.
- Keep this Instructions for Use and read it as needed.
- Each OMVOH prefilled Syringe is for one-time use only.
- Your healthcare provider can help you decide where on your body to inject your dose. Read the Choose and clean your injection sites section of these instructions to help you choose which area can work best for you.
- If you have vision problems, do not use OMVOH prefilled Syringes without help from a caregiver.
- See Storing OMVOH prefilled Syringes for important storage information.
INSTRUCTIONS FOR USE
Before you use the OMVOH prefilled Syringes, read and carefully follow all the step-by-step instructions.
2 Prefilled Syringes = full 300 mg dose
After your first injection, choose a new injection site at least 2 inches away and clean it.
With your second prefilled Syringe, repeat steps 1 to 3 right away after your first injection.
You must inject 2 prefilled Syringes to complete your full 300 mg dose.
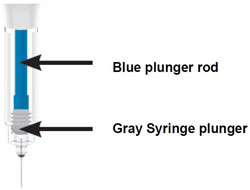
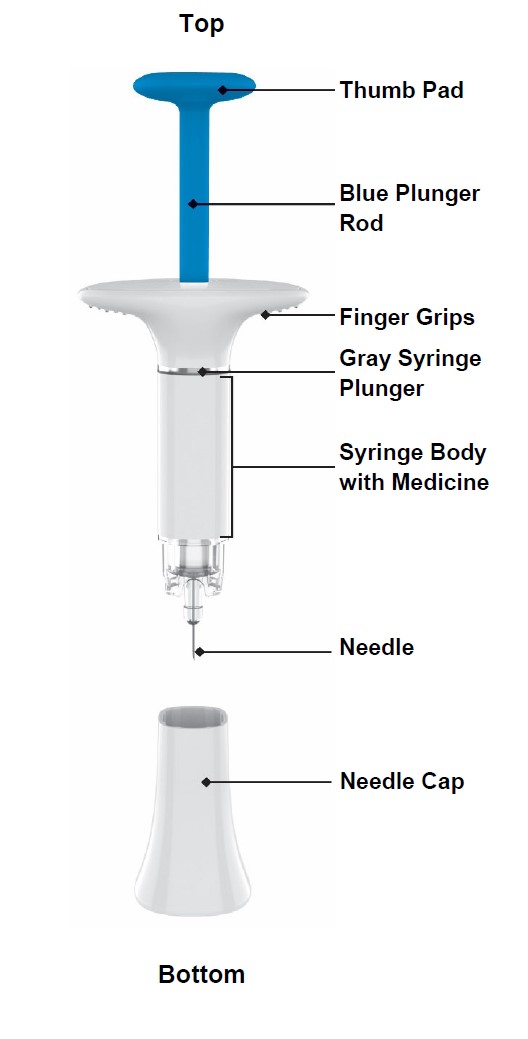
Parts of the OMVOH prefilled Syringes
Inject both prefilled Syringes in any order for a full 300 mg dose.
The 200 mg/2 mL (100 mg/mL) prefilled Syringe is larger than the 100 mg/mL prefilled Syringe.
Preparing to inject OMVOH
Gather supplies
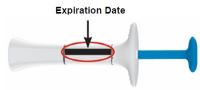
Inspect the prefilled Syringes and the medicine
Remove both prefilled Syringes from the carton.
Make sure you have the right medicine.
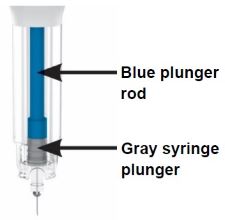
The medicine inside should be clear. It may be colorless to slightly yellow to slightly brown.
Wait 45 minutes
Do not warm up the prefilled Syringes with a microwave, hot water, or direct sunlight.
With the needle cap on, allow the prefilled Syringes to warm up to room temperature for 45 minutes before injecting.
Choose and clean your injection sites
Your healthcare provider can help you choose the injection sites that are best for you. Clean the injection sites with an alcohol wipe and let them dry.
Injecting OMVOH
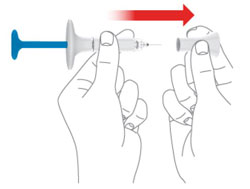
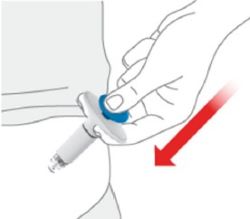
1. Uncap the first prefilled Syringe (the prefilled Syringes may be used in any order)
2. Pinch the injection site and insert the needle
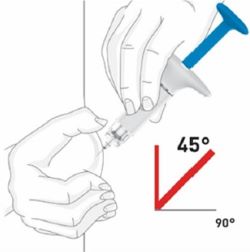
3. Inject the medicine
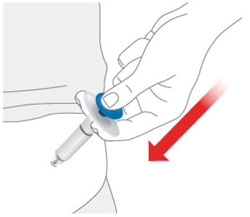
4. Inject the second prefilled Syringe
Choose a new injection site at least 2 inches away and clean it.
With your second prefilled Syringe, repeat steps 1 to 3 right away after your first injection.
You must inject 2 prefilled Syringes to complete your full 300 mg dose.
Throwing away (disposing of) OMVOH Prefilled Syringes
Throw away both used prefilled Syringes

Storing OMVOH Prefilled Syringes
Refrigeration
- In the original carton, store your prefilled Syringes in the refrigerator between 36°F to 46°F (2°C to 8°C) until the expiration date.
- Do not freeze. Do not use OMVOH if it has been frozen.
Room Temperature
- If needed, your prefilled Syringes may be stored at room temperature for up to 2 weeks in the original carton. Do not store above 86°F (30°C).
- When OMVOH has been stored at room temperature, do not return it to the refrigerator.
- Throw away (dispose of) OMVOH if not used within 2 weeks at room temperature.
- Protect your prefilled Syringes from light until use.
Do not use the prefilled Syringes and throw away (see Throwing away (disposing of) OMVOH Prefilled Syringes) if they have been:
Keep OMVOH and all medicines out of the reach of children.
Commonly asked questions
Additional Information:
If you have more questions about how to use the OMVOH prefilled Syringes:
Used OMVOH Prefilled Syringe disposal
Put the used OMVOH prefilled Syringes in an FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) the OMVOH prefilled Syringes in your household trash.
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container.
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container.
There may be state or local laws about how you should throw away needles and syringes.
For more information about safe sharps disposal, and for specific information about sharps disposal in the state you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
Do not recycle your used sharps disposal container.
Read the Medication Guide for OMVOH inside this box to learn more about your medicine.
Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOHTM is a trademark of Eli Lilly and Company.
Copyright © 2025, Eli Lilly and Company. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: January 2025
OMV-0001-300MG-PFS-IFU-20250115
200 MG PREFILLED PEN INSTRUCTIONS FOR USE



Throwing away (disposing of) OMVOH prefilled Pen

Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOH™ is a trademark of Eli Lilly and Company.
Copyright © 2025, Eli Lilly and Company. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: October 2025
The OMVOH prefilled Pen meets the current dose accuracy and functional requirements of ISO 11608-1 and 11608-5.
OMV-0001-200MG-PEN-IFU-20251023
200 MG PREFILLED SYRINGE INSTRUCTIONS FOR USE



Manufactured by:
Eli Lilly and Company
Indianapolis, IN 46285, USA
US License Number 1891
OMVOH is a trademark of Eli Lilly and Company.
Copyright © 2025, Eli Lilly and Company. All rights reserved.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: October 2025
OMV-0001-200MG-PFS-IFU-20251023
PACKAGE LABEL – Omvoh 300 mg Vial Cartons
There are two formulations for this product
NDC 0002-7575-01
15 mL
omvohTM
(mirikizumab-mrkz)
injection
300 mg/15 mL
(20 mg/mL)
For Intravenous Infusion After Dilution
Single-Dose Vial - Discard Unused Portion
Dispense enclosed Medication Guide to each patient.
Rx only
omvoh.com
Lilly
Classic Formulation contains the following inactive ingredients:anhydrous citric acid, polysorbate 80, sodium chloride, sodium citrate, and Water for Injection.
Alternate Formulation contains the following inactive ingredients: anhydrous citric acid, histidine, L-histidine hydrochloride monohydrate, mannitol, polysorbate 80, sodium chloride, sodium citrate, and Water for Injection.

PACKAGE LABEL – Omvoh Prefilled Pen 200 mg Dose Carton - Ulcerative Colitis
NDC 0002-8011-27
omvohTM
(mirikizumab-mrkz)
injection
100 mg/mL
For Subcutaneous Use Only
This carton contains a total dose of 200 mg.
Inject both prefilled pens one after the other for a full dose of 200 mg.
Note to Pharmacist: The entire carton is to be dispensed as a unit.
2 x 1 mL single-dose prefilled pens
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly
PACKAGE LABEL – Omvoh Prefilled Syringe 200 mg Dose Carton - Ulcerative Colitis
NDC 0002-8870-27
omvohTM
(mirikizumab-mrkz)
injection
100 mg/mL
For Subcutaneous Use Only
Note to Pharmacist: The entire carton is to be dispensed as a unit.
This carton contains a total dose of 200 mg.
Inject both prefilled syringes one after the other for a full dose of 200 mg.
2 x 1 mL single-dose prefilled syringes
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly
PACKAGE LABEL – Omvoh Prefilled Pen 300 mg Dose Carton - Crohns Disease
NDC 0002-7717-11
omvohTM
(mirikizumab-mrkz)
injection
200 mg/2 mL
100 mg/mL
For Subcutaneous Use Only
Note to Pharmacist: The entire carton is to be dispensed as a unit.
This carton contains a total dose of 300 mg.
Inject both prefilled pens one after the other for a full dose of 300 mg.
1 x 2 mL single-dose prefilled pen
1 x 1 mL single-dose prefilled pen
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly

PACKAGE LABEL – Omvoh Prefilled Syringe 300 mg Dose Carton - Crohns Disease
NDC 0002-7722-11
omvohTM
(mirikizumab-mrkz)
injection
200 mg/2 mL
(100 mg/mL)
100 mg/mL
For Subcutaneous Use Only
Note to Pharmacist: The entire carton is to be dispensed as a unit.
This carton contains a total dose of 300 mg.
Inject both prefilled syringes one after the other for a full dose of 300 mg.
1 x 2 mL single-dose prefilled syringe
1 x 1 mL single-dose prefilled syringe
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly
PACKAGE LABEL – Omvoh Prefilled Pen 200 mg Single Injection Dose Carton - Ulcerative Colitis
NDC 0002-3116-11
omvohTM
(mirikizumab-mrkz)
injection
200 mg/2 mL
For Subcutaneous Use Only
This carton contains a total dose of 200 mg.
Only one injection is required for a full dose.
1 x 200mg/2mL single dose prefilled pen
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly

PACKAGE LABEL – Omvoh Prefilled Syringe 200 mg Single Injection Dose Carton - Ulcerative Colitis
NDC 0002-1442-11
omvohTM
(mirikizumab-mrkz)
injection
200 mg/2 mL
(100 mg/mL)
For Subcutaneous Use Only
This carton contains a total dose of 200 mg.
Only one injection is required for a full dose.
1 x 200 mg/2 mL single-dose prefilled syringe
Rx only
Dispense enclosed Medication Guide to each patient.
Lilly
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.