TEZSPIRE (tezepelumab-ekko) injection, solution
Indications and Usage (1.2) 10/2025
1 INDICATIONS AND USAGE
TEZSPIRE is a thymic stromal lymphopoietin (TSLP) blocker, human monoclonal antibody (IgG2λ), indicated:
-
for the add-on maintenance treatment of adult and pediatric patients aged 12 years and older with severe asthma. (1.1) -
-
-
for the add-on maintenance treatment of adult and pediatric patients aged 12 years and older with inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP). (1.2)
1.1 Asthma
TEZSPIRE is indicated for the add-on maintenance treatment of adult and pediatric patients aged 12 years and older with severe asthma.
Limitations of Use:
TEZSPIRE is not indicated for the relief of acute bronchospasm or status asthmaticus.
1.2 Chronic Rhinosinusitis with Nasal Polyps
TEZSPIRE is indicated for the add-on maintenance treatment of adult and pediatric patients aged 12 years and older with inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP).
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
The recommended dosage of TEZSPIRE is 210 mg administered subcutaneously once every 4 weeks.
Missed Dose Information
If a dose is missed, administer the dose as soon as possible. Thereafter, the patient can continue (resume) dosing on the usual day of administration. If the next dose is already due, then administer as planned.
2.2 Preparation and Administration Instructions
TEZSPIRE vial and pre‑filled syringe are intended for administration by a healthcare provider.
TEZSPIRE pre-filled pen can be administered by patients/caregivers or healthcare providers. Patients/caregivers may administer TEZSPIRE pre-filled pen after proper training in subcutaneous injection technique and after the healthcare provider determines it is appropriate.
Each vial, pre-filled syringe and pre‑filled pen contain a single dose of TEZSPIRE.
-
Prior to administration, remove TEZSPIRE from the refrigerator and allow it to reach room temperature. This generally takes 60 minutes. Do not expose to heat and do not shake. Do not use if the security seal on the carton has been broken. Do not put back in the refrigerator once TEZSPIRE has reached room temperature. -
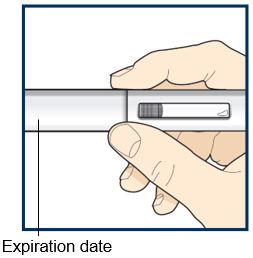
Visually inspect TEZSPIRE for particulate matter and discoloration prior to administration. TEZSPIRE is a clear to opalescent, colorless to light yellow solution. Do not use TEZSPIRE if liquid is cloudy, discolored, or if it contains large particles or foreign particulate matter. Do not use if the vial, pre-filled syringe or pre‑filled pen has been dropped or damaged or if the expiration date has passed. -
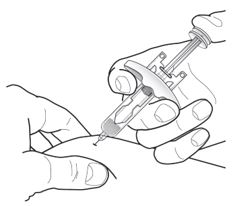
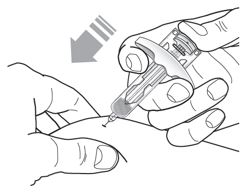
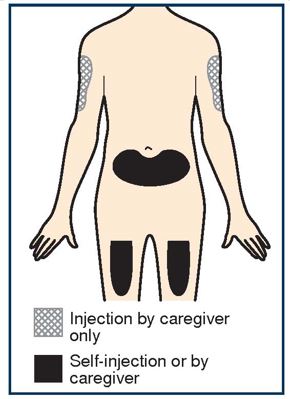
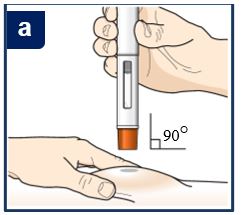
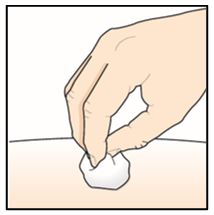
Inject TEZSPIRE 210 mg (contents of one vial, one pre-filled syringe or one pre-filled pen as described below) subcutaneously into the thigh or abdomen, except for the 2 inches (5 cm) around the navel. If a healthcare provider or caregiver administers the injection, the upper arm can also be used. A patient should not self-inject in the upper arm. TEZSPIRE should not be injected into areas where the skin is tender, bruised, erythematous, or hardened. It is recommended to rotate the injection site with each injection.
Administration Instructions for Single-Dose Pre-filled Syringe
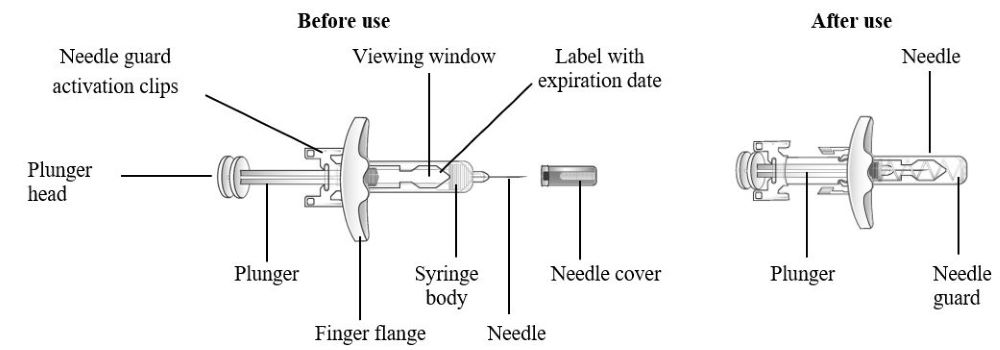
Refer to Figure 1 to identify the pre-filled syringe components for use in the administration steps.
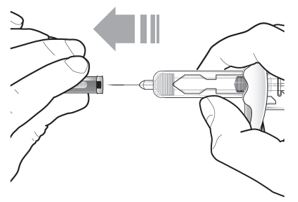
Do not remove the needle cover until Step 2 of these instructions when you are ready to inject TEZSPIRE. Do not touch the needle guard activation clips to prevent premature activation of the needle safety guard.
Figure 1 TEZSPIRE Pre-filled Syringe Components
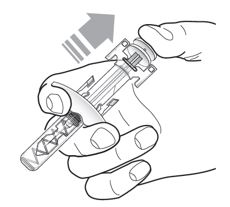
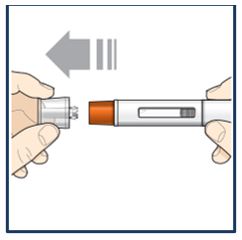
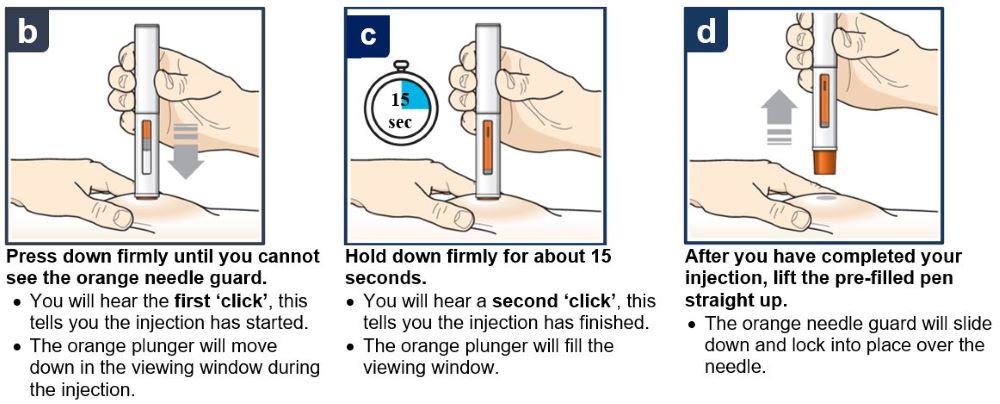
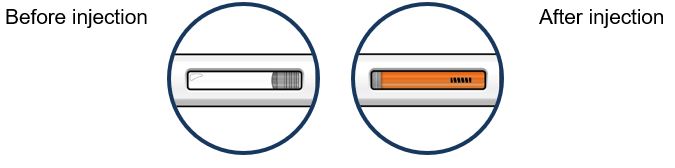
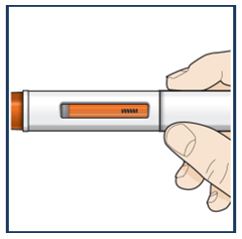
Administration Instructions for Single-Dose Pre-filled Pen
These administration instructions are intended for healthcare providers use only. Patients and caregivers should refer to the TEZSPIRE pre-filled pen ‘Instructions for Use’ for more detailed instructions on the preparation and administration of TEZSPIRE pre-filled pen [See Instructions for Use].
Patients/caregivers may inject after proper training in subcutaneous injection technique according to the ‘Instructions for Use’, and after the healthcare provider determines it is appropriate.
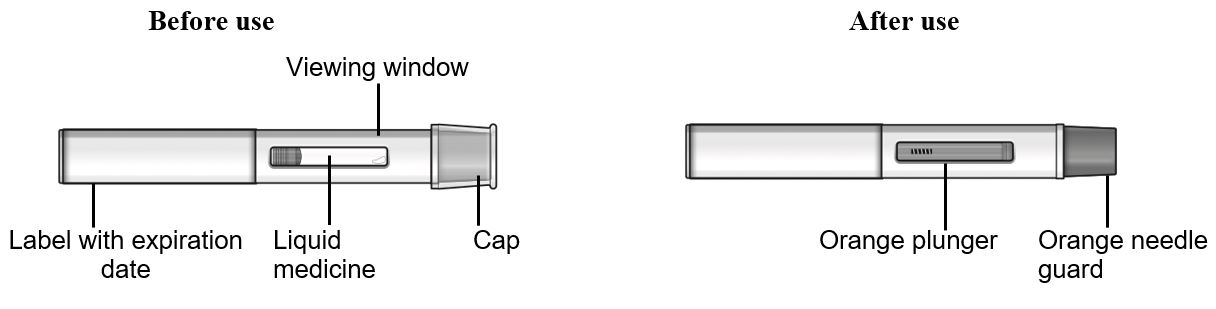
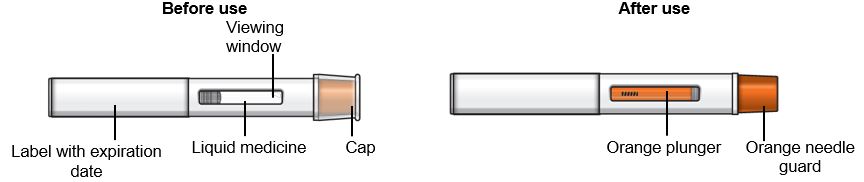
Refer to Figure 2 to identify the pre-filled pen components for use in the administration steps.
Do not remove the cap until you are ready to inject TEZSPIRE.
Figure 2 TEZSPIRE Pre-filled Pen Components





3 DOSAGE FORMS AND STRENGTHS
Injection: a clear to opalescent, colorless to light yellow solution available as:
-
210 mg/1.91 mL (110 mg/mL) solution in a single-dose glass vial. -
210 mg/1.91 mL (110 mg/mL) solution in a single-dose pre-filled syringe. -
210 mg/1.91 mL (110 mg/mL) solution in a single‑dose pre‑filled pen.
4 CONTRAINDICATIONS
TEZSPIRE is contraindicated in patients who have known hypersensitivity to tezepelumab-ekko or any of its excipients [see Warnings and Precautions (5.1)].
Known hypersensitivity to tezepelumab-ekko or excipients. (4)
5 WARNINGS AND PRECAUTIONS
-
Hypersensitivity Reactions: Hypersensitivity reactions have been observed in the clinical trials (e.g., rash, allergic conjunctivitis) following the administration of TEZSPIRE. Postmarketing cases of anaphylaxis have been reported. Initiate appropriate treatment as clinically indicated in the event of a hypersensitivity reaction. (5.1) -
Risk Associated with Abrupt Reduction in Corticosteroid Dosage: Do not discontinue systemic or inhaled corticosteroids abruptly upon initiation of therapy with TEZSPIRE. Decrease corticosteroids gradually, if appropriate. (5.3) -
Parasitic (Helminth) Infection: Treat patients with pre-existing helminth infections before therapy with TEZSPIRE. If patients become infected while receiving TEZSPIRE and do not respond to anti-helminth treatment, discontinue TEZSPIRE until the parasitic infection resolves. (5.4) -
Vaccination: Avoid use of live attenuated vaccines. (5.5)
5.1 Hypersensitivity Reactions
Hypersensitivity reactions were observed in the clinical trials (e.g., rash and allergic conjunctivitis) following the administration of TEZSPIRE. Postmarketing cases of anaphylaxis have also been reported [see Contraindications (4) and Adverse Reactions (6.2) ]. These reactions can occur within hours of administration, but in some instances have a delayed onset (i.e., days). In the event of a hypersensitivity reaction, consider the benefits and risks for the individual patient to determine whether to continue or discontinue treatment with TEZSPIRE.
5.2 Acute Asthma Symptoms or Deteriorating Disease
TEZSPIRE should not be used to treat acute asthma symptoms or acute exacerbations. Do not use TEZSPIRE to treat acute bronchospasm or status asthmaticus. Patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with TEZSPIRE.
5.3 Risk Associated with Abrupt Reduction of Corticosteroid Dosage
Do not discontinue systemic or inhaled corticosteroids abruptly upon initiation of therapy with TEZSPIRE. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a physician. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
5.4 Parasitic (Helminth) Infection
Thymic stromal lymphopoietin (TSLP) may be involved in the immunological response to some helminth infections. Patients with known helminth infections were excluded from participation in clinical trials. It is unknown if TEZSPIRE will influence a patient’s response against helminth infections.
Treat patients with pre-existing helminth infections before initiating therapy with TEZSPIRE. If patients become infected while receiving treatment with TEZSPIRE and do not respond to anti-helminth treatment, discontinue treatment with TEZSPIRE until infection resolves.
5.5 Live Attenuated Vaccines
The concomitant use of TEZSPIRE and live attenuated vaccines has not been evaluated. The use of live attenuated vaccines should be avoided in patients receiving TEZSPIRE.
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
-
Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
Most common adverse reactions (incidence ≥ 3%) are:
-
Asthma: pharyngitis, arthralgia, and back pain. (6.1) -
Chronic rhinosinusitis with nasal polyps: nasopharyngitis, upper respiratory tract infection, epistaxis, pharyngitis, back pain, influenza, injection site reaction and arthralgia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca at 1-800-236-9933 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse Reactions in Adult and Pediatric Patients 12 Years of Age and Older with Asthma
The safety of TEZSPIRE in asthma was based on the pooled safety population from PATHWAY and NAVIGATOR, which consists of 665 adult and pediatric patients 12 years of age and older with severe asthma who received at least one dose of TEZSPIRE 210 mg subcutaneously once every 4 weeks. The two placebo-controlled clinical trials were of 52 weeks duration. In addition, a similar safety profile was seen in a trial that enrolled 150 adult patients with severe asthma who required treatment with daily oral corticosteroids [see Clinical Studies (14.1) ].
Adverse reactions that occurred at an incidence greater than or equal to 3% and more common than in the placebo group from the pooled safety population (PATHWAY and NAVIGATOR) are shown in Table 1.
Specific Adverse Reactions
Cardiovascular Events
In a randomized, double-blind, long term extension trial, patients 12 years and older with severe asthma from trials NAVIGATOR and the additional trial [see Clinical Studies (14.1)] received TEZSPIRE 210 mg subcutaneously every 4 weeks or placebo for up to 104 weeks. In the trial, the incidence rates (IR) per 100 patient-years (PY) for serious cardiac adverse events in patients treated with TEZSPIRE or placebo were 1.08 and 0.21, respectively, with an incidence rate difference (IRD) of 0.88 (95% CI: 0.24, 1.53). The types of serious cardiac adverse events were heterogeneous. In the trial, the IR per 100 PY for adjudicated major adverse cardiovascular events (MACE, defined as cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) in patients treated with TEZSPIRE or placebo were 0.60 and 0.42, respectively, with an IRD of 0.18 (95% CI: -0.51, 0.75).
Injection Site Reactions
In the pooled safety population (PATHWAY and NAVIGATOR), in which TEZSPIRE or placebo was administered using the vial by a healthcare provider, injection site reactions (e.g., injection site erythema, injection site swelling, injection site pain) occurred at a rate of 3.3% in patients treated with TEZSPIRE compared with 2.7% in patients treated with placebo.
In an open-label trial of 216 patients with asthma in which TEZSPIRE was administered by healthcare providers and patients or caregivers using either the pre-filled pen or pre-filled syringe, injection site reactions (e.g., injection site erythema, injection site swelling, injection site pain) were observed in 5.7% patients using the pre-filled pen and 0% using the pre-filled syringe. However, the trial was not designed to compare injection site reactions between patients who received TEZSPIRE by the pre-filled pen versus pre-filled syringe.
Adverse Reactions in Adult Patients with Chronic Rhinosinusitis with Nasal Polyps
The safety of TEZSPIRE in CRSwNP was based on WAYPOINT, a randomized, double-blind, parallel group, multicenter, placebo-controlled trial of 52 weeks duration, which consisted of 203 adult patients aged 18 years and older on standard of care treatment for CRSwNP who received at least one dose of TEZSPIRE 210 mg subcutaneously once every 4 weeks [see Clinical Studies (14.2)].
Adverse reactions that occurred at an incidence greater than or equal to 3% and more common than in the placebo group from the safety population (WAYPOINT) are shown in Table 2.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of TEZSPIRE. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hypersensitivity reactions: anaphylaxis
7 DRUG INTERACTIONS
No formal drug interaction studies have been performed with TEZSPIRE.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on TEZSPIRE use in pregnant women to evaluate for any drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. Placental transfer of monoclonal antibodies such as tezepelumab-ekko is greater during the third trimester of pregnancy; therefore, potential effects on a fetus are likely to be greater during the third trimester of pregnancy. In an enhanced pre- and post-natal development (ePPND) study conducted in cynomolgus monkeys, placental transport of tezepelumab-ekko was observed but there was no evidence of fetal harm following intravenous administration of tezepelumab-ekko throughout pregnancy at doses that produced maternal exposures up to 168 times the exposure at the maximum recommended human dose (MRHD) of 210 mg administered subcutaneously (see Data).
The estimated background risk of major birth defects and miscarriages for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk:
In women with poorly or moderately controlled asthma, evidence demonstrates that there is an increased risk of preeclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. The level of asthma control should be closely monitored in pregnant women and treatment adjusted as necessary to maintain optimal control.
Data
Animal Data
In the ePPND study, pregnant cynomolgus monkeys received tezepelumab-ekko from GD20 to GD22 (dependent on pregnancy determination), at the beginning of organogenesis, and once every 7 days until the end of gestation at doses that produced exposures up to 168 times that achieved with the MRHD (on an AUC basis with maternal intravenous doses up to 300 mg/kg/week). There were no tezepelumab-ekko related adverse effects on maternal health, pregnancy outcome, embryo-fetal development, or neonatal growth and development up to 6.5 months of age. Tezepelumab-ekko crossed the placenta in cynomolgus monkeys and tezepelumab-ekko serum concentrations were 0.5- to 6.7-fold higher in infants relative to maternal animals.
8.2 Lactation
Risk Summary
There is no information regarding the presence of tezepelumab-ekko in human milk, its effects on the breastfed infant, or its effects on milk production. However, tezepelumab-ekko is a human monoclonal antibody immunoglobulin G2λ (IgG2λ), and immunoglobulin G (IgG) is present in human milk in small amounts. Tezepelumab‑ekko was present in the milk of cynomolgus monkeys postpartum following dosing during pregnancy (see Data). The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for TEZSPIRE and any potential adverse effects on the breastfed infant from TEZSPIRE or from the underlying maternal condition.
Data
Animal Data
In a prenatal and postnatal development study in cynomolgus monkeys, tezepelumab-ekko concentrations in milk were up to 0.5% of the maternal serum concentrations after intravenous administration of tezepelumab-ekko up to 300 mg/kg/week (168 times the exposures based on AUC achieved at MRHD). The concentration of tezepelumab-ekko in animal milk does not necessarily predict the concentration of drug in human milk.
8.4 Pediatric Use
Asthma
The safety and effectiveness of TEZSPIRE for the add-on maintenance treatment of severe asthma have been established in pediatric patients aged 12 years and older [see Adverse Reactions (6.1) and Clinical Studies (14.1)] . Use of TEZSPIRE for this indication is supported by evidence from a total of 82 pediatric patients aged 12 to 17 years enrolled in NAVIGATOR and received treatment with TEZSPIRE 210 mg subcutaneously every 4 weeks (n=41) or placebo (n=41). Compared with placebo, improvements in annualized asthma exacerbation (rate ratio 0.70; 95% CI 0.34, 1.46) and FEV1 (LS mean change versus placebo 0.17 L; 95% CI -0.01, 0.35) were observed in pediatric patients treated with TEZSPIRE. The safety profile and pharmacodynamic responses in pediatric patients were generally similar to the overall study population.
The safety and effectiveness of TEZSPIRE have not been established in patients younger than 12 years of age with asthma.
CRSwNP
The safety and effectiveness of TEZSPIRE for the add-on maintenance treatment of inadequately controlled CRSwNP have been established in pediatric patients aged 12 years and older. Use of TEZSPIRE for this indication is supported by evidence from the adequate and well-controlled study of TEZSPIRE in adults (WAYPOINT) [see Clinical Studies (14.2)] with the following additional data:
-
Pharmacokinetic (PK) data from adult and pediatric patients aged 12 years and older with severe asthma and adult patients with CRSwNP [see Clinical Pharmacology (12.3)]. -
Safety data in pediatric patients aged 12 years and older with severe asthma [see Adverse Reactions (6.1)].
The safety and effectiveness of TEZSPIRE have not been established in patients younger than 12 years of age with CRSwNP.
8.5 Geriatric Use
Asthma
Of the 665 patients with asthma treated with TEZSPIRE in clinical trials (PATHWAY and NAVIGATOR) for severe asthma, 119 patients (18%) were 65 years or older. No overall differences in safety or effectiveness of TEZSPIRE have been observed between patients 65 years of age and older and younger patients [see Adverse Reactions (6.1) and Clinical Studies (14.1) ].
CRSwNP
Of the 203 patients with CRSwNP treated with TEZSPIRE in a clinical trial (WAYPOINT) for CRSwNP, 29 patients (14%) were 65 years or older. No overall differences in safety or effectiveness of TEZSPIRE have been observed between patients 65 years of age and older and younger adult patients [see Adverse Reactions (6.1) and Clinical Studies (14.2)].
11 DESCRIPTION
Tezepelumab-ekko, a thymic stromal lymphopoietin (TSLP) blocker, is a human monoclonal antibody immunoglobulin G2λ (IgG2λ) produced in Chinese hamster ovary (CHO) cells by recombinant DNA technology. Tezepelumab-ekko has a molecular weight of approximately 147 kDa.
TEZSPIRE (tezepelumab-ekko) injection is a sterile, preservative-free, clear to opalescent, colorless to light yellow solution for subcutaneous injection supplied in a single-dose vial, single-dose pre-filled syringe or single‑dose pre‑filled pen.
Each single-dose vial, pre-filled syringe or pre‑filled pen delivers 1.91 mL containing 210 mg tezepelumab-ekko, glacial acetic acid (2.8 mg), L-proline (48 mg), polysorbate 80 (0.19 mg), sodium hydroxide, and water for injection. The pH is 5.2.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Tezepelumab-ekko is a thymic stromal lymphopoietin (TSLP) blocker, human monoclonal antibody IgG2λ that binds to human TSLP with a dissociation constant of 15.8 pM and blocks its interaction with the heterodimeric TSLP receptor. TSLP is a cytokine mainly derived from epithelial cells and occupies an upstream position in inflammatory cascades.
Airway and mucosal inflammation are important components of the pathogenesis of asthma and CRSwNP. Multiple cell types (e.g., mast cells, eosinophils, neutrophils, macrophages, lymphocytes, ILC2 cells) and mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines) are involved in airway and mucosal inflammation. Increased levels of TSLP mRNA and protein are found in the airways of patients with asthma as well as in nasal polyp tissue. Blocking TSLP with tezepelumab-ekko reduces biomarkers and cytokines associated with inflammation including blood eosinophils, airway submucosal eosinophils, IgE, FeNO, IL-5, and IL-13; however, the mechanism of tezepelumab-ekko action in asthma and CRSwNP has not been definitively established.
12.2 Pharmacodynamics
In NAVIGATOR, administration of TEZSPIRE 210 mg subcutaneously every 4 weeks (n=528) reduced blood eosinophils counts, FeNO, IL-5 concentration and IL-13 concentration from baseline compared with placebo (n=531) with an onset of effect 2 weeks after initiation of treatment and sustained reduction on treatment to 52 weeks. TEZSPIRE caused a slow but progressive reduction in serum total IgE concentration throughout 52 weeks of treatment. Similar effects were seen in PATHWAY.
In WAYPOINT, administration of TEZSPIRE 210 mg subcutaneously every 4 weeks (n=203) resulted in reductions from baseline of blood eosinophils, FeNO (in participants with co-morbid asthma [about 60% of patients]) and serum IgE as compared to placebo (n=205). Blood eosinophils were reduced beginning at Week 4, the first observed timepoint, with reductions maintained through Week 52. Reductions in FeNO and serum IgE were observed during the treatment period at Weeks 24 and 52.
12.3 Pharmacokinetics
The pharmacokinetics of tezepelumab-ekko is similar in patients with asthma and CRSwNP.
The pharmacokinetics of tezepelumab-ekko were dose-proportional following administration of a single subcutaneous dose over a dose range from 0.01 to 2 times the recommended dose. With an every 4 weeks dosing regimen, tezepelumab-ekko achieves steady-state after 12 weeks and the accumulation ratio for Ctrough is 1.86-fold.
Absorption
Following subcutaneous administration, the maximum serum concentration was reached in approximately 3 to 10 days. Based on population pharmacokinetic analysis, the estimated absolute bioavailability was approximately 77%. There was no clinically relevant difference in bioavailability when administered to different injection sites (abdomen, thigh, or upper arm).
Distribution
Based on population pharmacokinetic analysis, central and peripheral volume of distribution of tezepelumab-ekko were 3.9 L and 2.2 L, respectively, for a 70 kg individual.
Elimination
As a human monoclonal antibody, tezepelumab-ekko is eliminated by intracellular catabolism and there is no evidence of target-mediated clearance within the studied dose range. Based on population pharmacokinetic analysis, the estimated clearance for tezepelumab-ekko was 0.17 L/d for a 70 kg individual. The elimination half-life was approximately 26 days.
Metabolism
Tezepelumab-ekko is a human monoclonal antibody (IgG2λ) that is degraded by proteolytic enzymes widely distributed in the body and not metabolized by hepatic enzymes.
Specific Populations
Age, Sex, Race
Based on population pharmacokinetic analysis, age (12 to 80 years), sex and race (White, Black, Asian, Other) had no clinically meaningful effects on the pharmacokinetics of tezepelumab-ekko.
Body Weight
Based on population pharmacokinetic analysis, higher body weight was associated with lower exposure. However, the effect of body weight on exposure had no meaningful impact on efficacy or safety and does not require dose adjustment.
Pediatric Patients
CRSwNP
Clinical studies have not been conducted in pediatric patients aged 12 years and older with CRSwNP. Tezepelumab-ekko exposures are expected to be comparable between adults and pediatric patients aged 12 years and older at the recommended subcutaneous dosage (210 mg every 4 weeks) for CRSwNP.
Patients with Renal impairment
No formal clinical studies have been conducted to investigate the effect of renal impairment on tezepelumab-ekko. The population pharmacokinetic analysis included 320 (23%) subjects with mild renal impairment and 38 (3%) subjects with moderate renal impairment. Tezepelumab-ekko clearance was similar in patients with mild renal impairment (estimated creatinine clearance 60 to 89 mL/min), moderate renal impairment (estimated creatinine clearance 30 to 59 mL/min) and those with normal renal function (estimated creatinine clearance ≥ 90 mL/min). Tezepelumab-ekko has not been studied in patients with severe renal impairment (estimated creatinine clearance < 30 mL/min).
Patients with Hepatic impairment
No formal clinical studies have been conducted to investigate the effect of hepatic impairment on tezepelumab-ekko. Since tezepelumab-ekko is degraded by proteolytic enzymes widely distributed in the body and not metabolized by hepatic-specific enzymes, change in hepatic function is not expected to influence tezepelumab-ekko clearance.
Drug Interaction Studies
No formal drug interaction studies have been conducted with tezepelumab-ekko. Based on the population pharmacokinetic analysis, commonly co-administered asthma medications (leukotriene receptor antagonist, theophylline/aminophylline, oral and inhaled corticosteroid) had no clinically meaningful effect on tezepelumab-ekko clearance.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies, including those of tezepelumab-ekko or of other tezepelumab products.
In patients with asthma (NAVIGATOR and an additional trial), anti-drug antibodies (ADA) were detected at any time in 29 (5%) out of 601 patients who received TEZSPIRE at the recommended dosing regimen during the 48 to 52‑week study period. Of these 29 patients, 11 patients (2% of patients treated with TEZSPIRE) developed treatment-emergent antibodies and 1 patient (<1% of patients treated with TEZSPIRE) developed neutralizing antibodies. ADA titers were generally low and often transient. No evidence of ADA impact on pharmacokinetics, pharmacodynamics, efficacy, or safety was observed.
In patients with CRSwNP (WAYPOINT), a treatment-emergent ADA response developed in 5 (3%) out of 164 patients treated with TEZSPIRE at the recommended dosage regimen during the 52-week treatment period. Neutralizing antibodies were detected in 1 of the ADA positive patients. While there was no observed impact of ADA on pharmacokinetics, pharmacodynamics, efficacy, or safety, there were insufficient numbers of patients with treatment‑emergent ADA to make a formal assessment in CRSwNP.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Animal studies have not been conducted to evaluate the carcinogenic potential of tezepelumab-ekko. The malignancy risk in humans from an antibody that blocks TSLP ligand, such as tezepelumab-ekko, is currently unknown.
Male and female fertility was unaffected based upon no observed adverse histopathological findings in the reproductive organs and no changes in menstrual cycle or semen analysis in sexually mature cynomolgus monkeys that received tezepelumab-ekko for 26 weeks at subcutaneous doses up to 300 mg/kg/week (approximately 134 times the MRHD on an AUC basis).
14 CLINICAL STUDIES
14.1 Clinical Studies in Patients with Asthma
The efficacy of TEZSPIRE for add-on maintenance treatment of severe asthma was evaluated in two randomized, double-blind, parallel group, placebo-controlled clinical trials (PATHWAY [NCT02054130] and NAVIGATOR [NCT03347279]) of 52 weeks duration. The two trials enrolled a total of 1,609 patients 12 years of age and older with severe asthma.
PATHWAY was a 52-week dose-ranging exacerbation trial that enrolled 550 adult patients with severe asthma who received treatment with tezepelumab-ekko 70 mg subcutaneously every 4 weeks, TEZSPIRE 210 mg subcutaneously every 4 weeks, tezepelumab-ekko 280 mg subcutaneously every 2 weeks, or placebo subcutaneously. Patients were required to have a history of 2 or more asthma exacerbations requiring oral or injectable corticosteroid treatment or 1 asthma exacerbation resulting in hospitalization in the past 12 months.
NAVIGATOR was a 52-week exacerbation trial that enrolled 1,061 patients (adult and pediatric patients 12 years of age and older) with severe asthma who received treatment with TEZSPIRE 210 mg subcutaneously every 4 weeks or placebo subcutaneously every 4 weeks. Patients were required to have a history of 2 or more asthma exacerbations requiring oral or injectable corticosteroid treatment or resulting in hospitalization in the past 12 months.
In both PATHWAY and NAVIGATOR, patients were required to have an Asthma Control Questionnaire 6 (ACQ-6) score of 1.5 or more at screening and reduced lung function at baseline [pre-bronchodilator forced expiratory volume in 1 second (FEV1) below 80% predicted in adults, and below 90% predicted in adolescents]. Patients were required to have been on regular treatment with medium or high-dose inhaled corticosteroids (ICS) and at least one additional asthma controller, with or without oral corticosteroids (OCS). Patients continued background asthma therapy throughout the duration of the trials. In both trials, patients were enrolled without requiring a minimum baseline level of blood eosinophils or FeNO.
The demographics and baseline characteristics of PATHWAY and NAVIGATOR are provided in Table 3 below.
Table 3 Demographics and Baseline Characteristics of Patients in PATHWAY and NAVIGATOR
EOS, Eosinophils; FEIA, Fluorescent enzyme immunoassay; FeNO, Fractional exhaled nitric oxide; FEV1, Forced expiratory volume in one second; ICS, Inhaled corticosteroid, IgE, Immunoglobulin E; OCS, Oral corticosteroid; ppb, Parts per billion; SD, Standard deviation
The results summarized below are for the recommended TEZSPIRE 210 mg subcutaneously every 4 weeks dosing regimen.
Exacerbations
The primary endpoint for PATHWAY and NAVIGATOR was the rate of clinically significant asthma exacerbations measured over 52 weeks. Clinically significant asthma exacerbations were defined as worsening of asthma requiring the use of or increase in oral or injectable corticosteroids for at least 3 days, or a single depo-injection of corticosteroids, and/or emergency department visits requiring use of oral or injectable corticosteroids and/or hospitalization.
In both PATHWAY and NAVIGATOR, patients receiving TEZSPIRE had significant reductions in the annualized rate of asthma exacerbations compared to placebo. There were also fewer exacerbations requiring emergency room visits and/or hospitalization in patients treated with TEZSPIRE compared with placebo (Table 4).
Table 4 Rate of Clinically Significant Exacerbations Over 52 Weeks in PATHWAY and NAVIGATOR
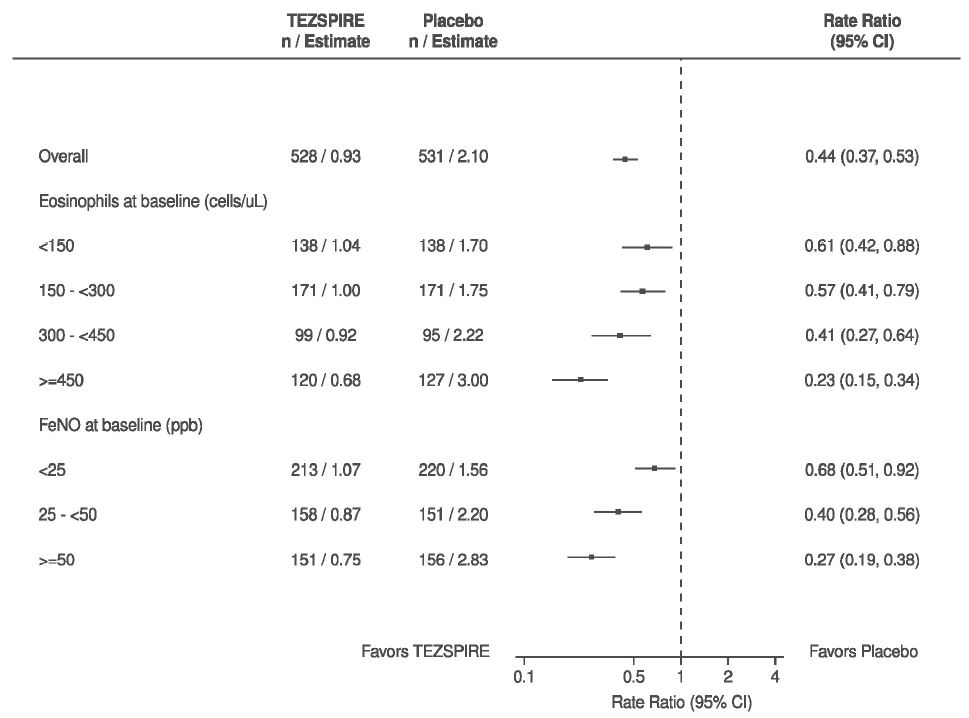
In NAVIGATOR, patients receiving TEZSPIRE experienced fewer exacerbations than those receiving placebo regardless of baseline levels of blood eosinophils or FeNO (Figure 3). Similar results were seen in PATHWAY.
Figure 3 Annualized Asthma Exacerbation Rate Ratio Over 52 Weeks Across Different Baseline Biomarkers in NAVIGATOR
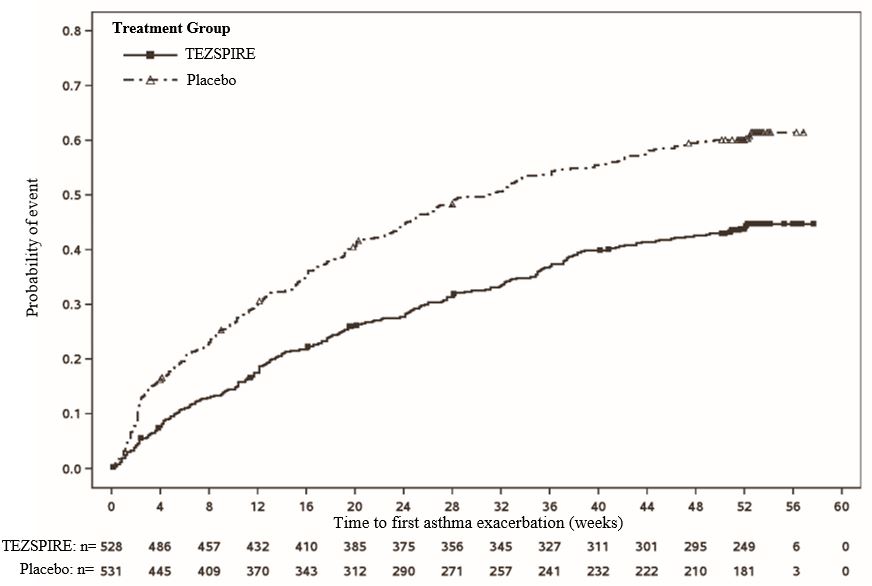
The time to first exacerbation was longer for the patients receiving TEZSPIRE compared with placebo in NAVIGATOR (Figure 4). Similar findings were seen in PATHWAY.
Figure 4 Kaplan-Meier Cumulative Incidence Curves for Time to First Exacerbation in NAVIGATOR
Lung Function
Change from baseline in FEV1 was assessed as a secondary endpoint in PATHWAY and NAVIGATOR. Compared with placebo, TEZSPIRE provided clinically meaningful improvements in the mean change from baseline in FEV1 in both trials (Table 5).
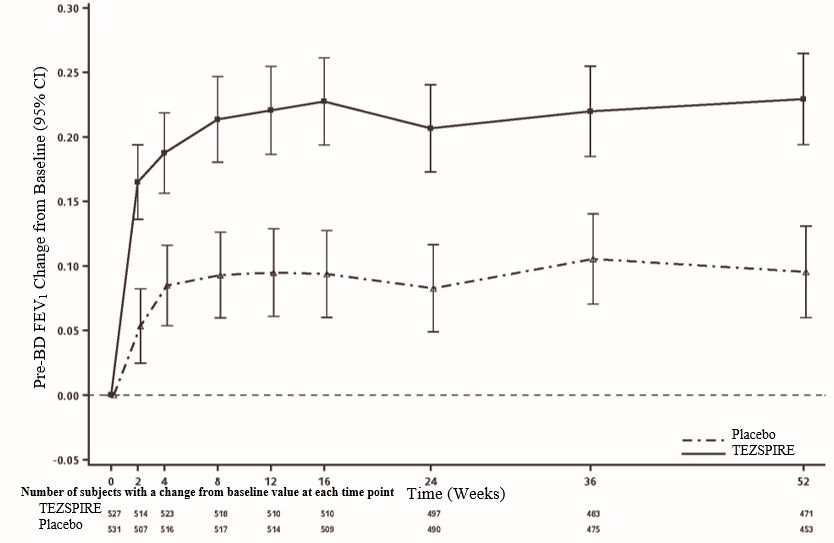
In NAVIGATOR, improvement in FEV1 was seen as early as 2 weeks after initiation of treatment and was sustained through week 52 (Figure 5).
Figure 5 Mean Change (95% CI) from Baseline in Pre-Bronchodilator FEV1 (L) in NAVIGATOR
Patient Reported Outcomes
Changes from baseline in Asthma Control Questionnaire 6 (ACQ-6) and Standardized Asthma Quality of Life Questionnaire for ages 12 and older [AQLQ(S)+12] were also assessed as secondary endpoints in PATHWAY and NAVIGATOR. In both trials, more patients treated with TEZSPIRE compared to placebo had a clinically meaningful improvement in ACQ-6 and AQLQ(S)+12. Clinically meaningful improvement (responder rate) for both measures was defined as improvement in score of 0.5 or more at end of trial. In NAVIGATOR, the ACQ-6 responder rate for TEZSPIRE was 86% compared with 77% for placebo (OR=1.99; 95% CI 1.43, 2.76) and the AQLQ(S)+12 responder rate for TEZSPIRE was 78% compared with 72% for placebo (OR=1.36; 95% CI 1.02, 1.82). Similar findings were seen in PATHWAY.
Additional Trial
In a randomized, double-blind, parallel group, placebo-controlled clinical trial, the effect of TEZSPIRE (210 mg subcutaneously every 4 weeks) on reducing the use of maintenance OCS was evaluated. The trial enrolled 150 adult patients with severe asthma who required treatment with daily OCS (7.5 mg to 30 mg per day) in addition to regular use of high-dose ICS and a long-acting beta-agonist with or without additional controller(s). The primary endpoint was categorized percent reduction from baseline of the final OCS dose at Week 48 (≥90% reduction, ≥75% to <90% reduction, ≥50% to <75% reduction, >0% to <50% reduction, and no change or any increase in OCS), while maintaining asthma control. TEZSPIRE did not demonstrate a statistically significant reduction in maintenance OCS dose compared with placebo (cumulative OR=1.28; 95% CI 0.69, 2.35).
14.2 Clinical Studies in Patients with Chronic Rhinosinusitis with Nasal Polyps
The efficacy of TEZSPIRE for add-on maintenance treatment of inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP) was evaluated in a randomized, double-blind, parallel group, multicenter, placebo-controlled trial (WAYPOINT [NCT04851964]) of 52 weeks treatment duration conducted in 408 patients aged 18 years and older on standard of care treatment for CRSwNP. This study included patients with symptomatic CRSwNP despite treatment with nasal corticosteroids, and who had systemic corticosteroids within the past 12 months and/or any history of sino-nasal surgery, or with contraindications and/or intolerance to either.
Patients received TEZSPIRE 210 mg or placebo subcutaneously every 4 weeks for 52 weeks in addition to nasal corticosteroid treatment for CRSwNP.
The demographics and baseline characteristics of patients enrolled in WAYPOINT are provided in Table 6.
AERD, Aspirin exacerbated respiratory disease; CRSwNP, Chronic rhinosinusitis with nasal polyps; CT, Computed tomography; IgE, Immunoglobulin E; IU, International units; LMK, Lund-Mackay; NCS, Nasal congestion score; NPS, Nasal polyp score; NSAID‑ERD, Nonsteroidal anti-inflammatory drug exacerbated respiratory disease; SD, Standard deviation
The co-primary efficacy endpoints were change from baseline in total nasal polyp score (NPS) evaluated by nasal endoscopy at Week 52 as graded by independent blinded assessors, and change from baseline in bi-weekly mean nasal congestion score (NCS) evaluated at Week 52. For total NPS, polyps on each side of the nose were graded on a categorical scale (0=no polyps, 1=small polyps in the middle meatus not reaching below the inferior border of the middle turbinate, 2=polyps reaching below the lower border of the middle turbinate, 3=polyps reaching the lower border of the inferior turbinate or a middle meatal polyp with a score of 2 with any additional polyp medial to the middle turbinate, 4=large polyps causing complete or near complete obstruction of the inferior nasal cavity [i.e. touching the floor of the nose]) for a total score of 0 to 8. Nasal congestion was rated daily by the patients on a 0 to 3 categorical severity scale (0=none, 1=mild, 2=moderate, 3=severe).
Statistically significant efficacy was observed in WAYPOINT for the co-primary endpoints of improvement in total NPS and in bi-weekly mean NCS at Week 52 (Table 7).
Figure 6 demonstrates the time course of improvement in the mean change from baseline in NPS.
Figure 6 LS Mean Change from Baseline in Total Nasal Polyp Score up to Week 52 in Adults (WAYPOINT)
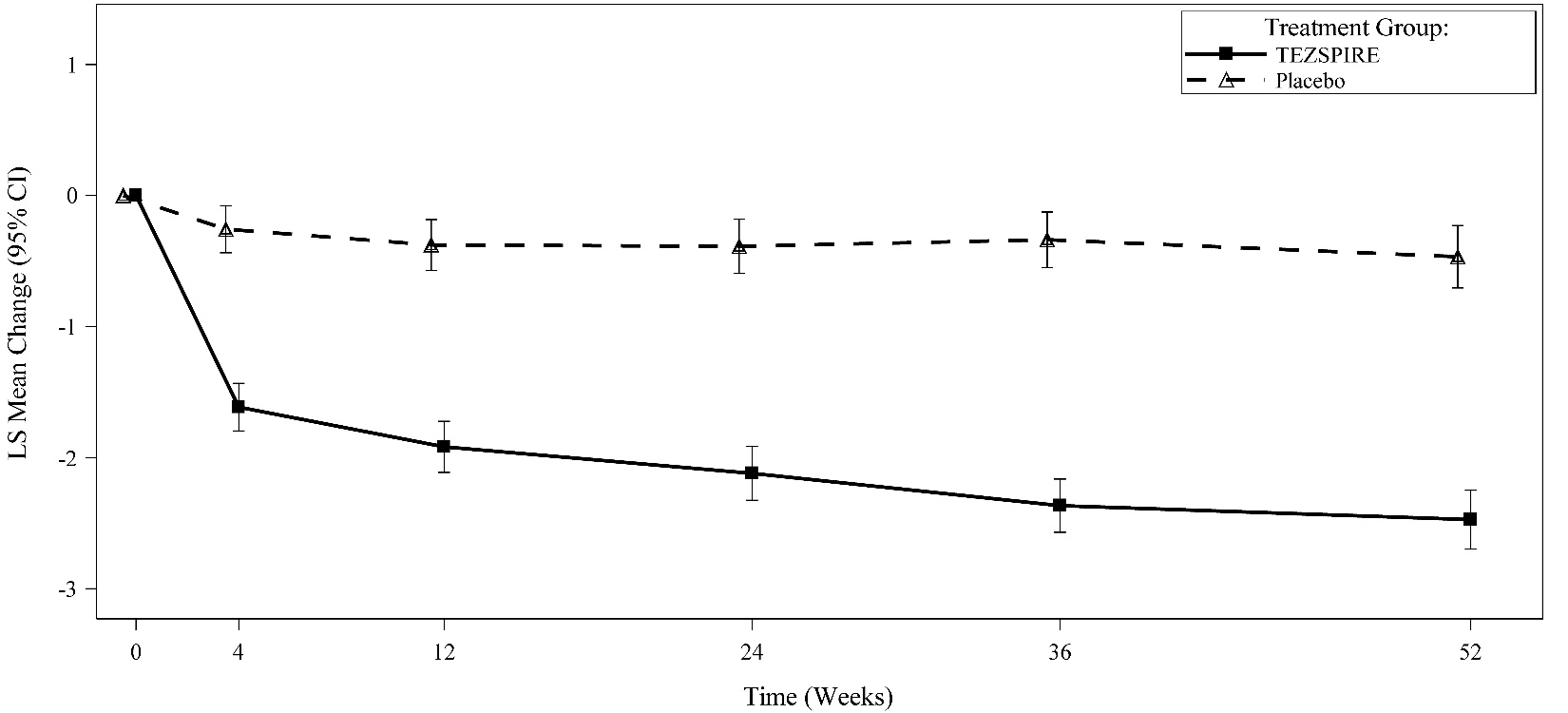
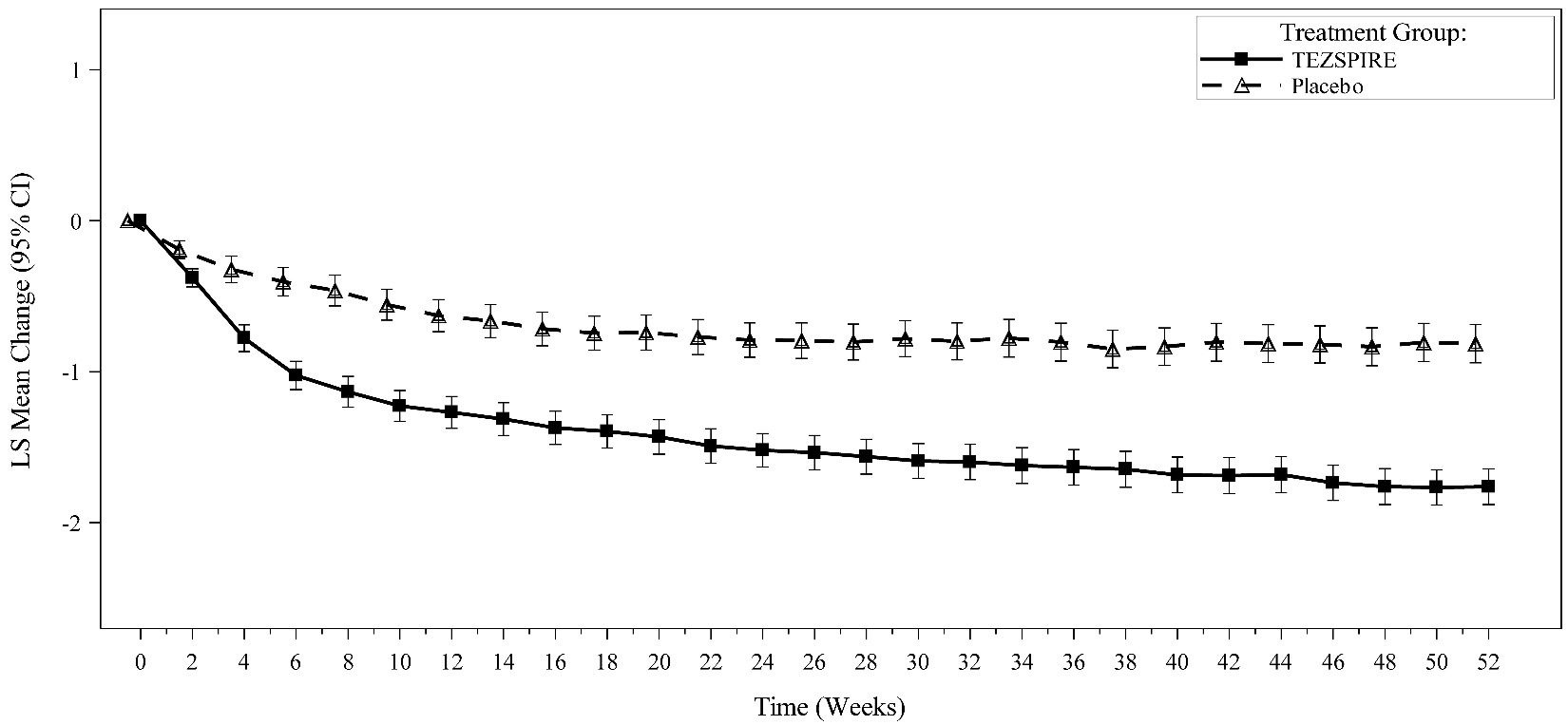
Figure 7 demonstrates the time course of improvement in the bi-weekly mean change from baseline in NCS.
Figure 7 LS Mean Change from Baseline in Bi-weekly Mean Nasal Congestion Score up to Week 52 in Adults (WAYPOINT)
Key secondary endpoints at Week 52 included time to surgery decision and/or systemic corticosteroid use for nasal polyps, change from baseline in loss of smell, and change from baseline in Lund-Mackay (LMK) sinus CT scan score.
TEZSPIRE significantly reduced the proportion of patients with need for sino-nasal surgery or systemic corticosteroids by 92% compared to placebo over 52 weeks (Hazard Ratio: 0.08; 95% CI: 0.03, 0.17) (Figure 8).
Figure 8 Kaplan Meier Curve for Time to First Systemic Corticosteroid Use and/or Sino-Nasal Surgery Decision Over 52 Weeks in Adults (WAYPOINT)
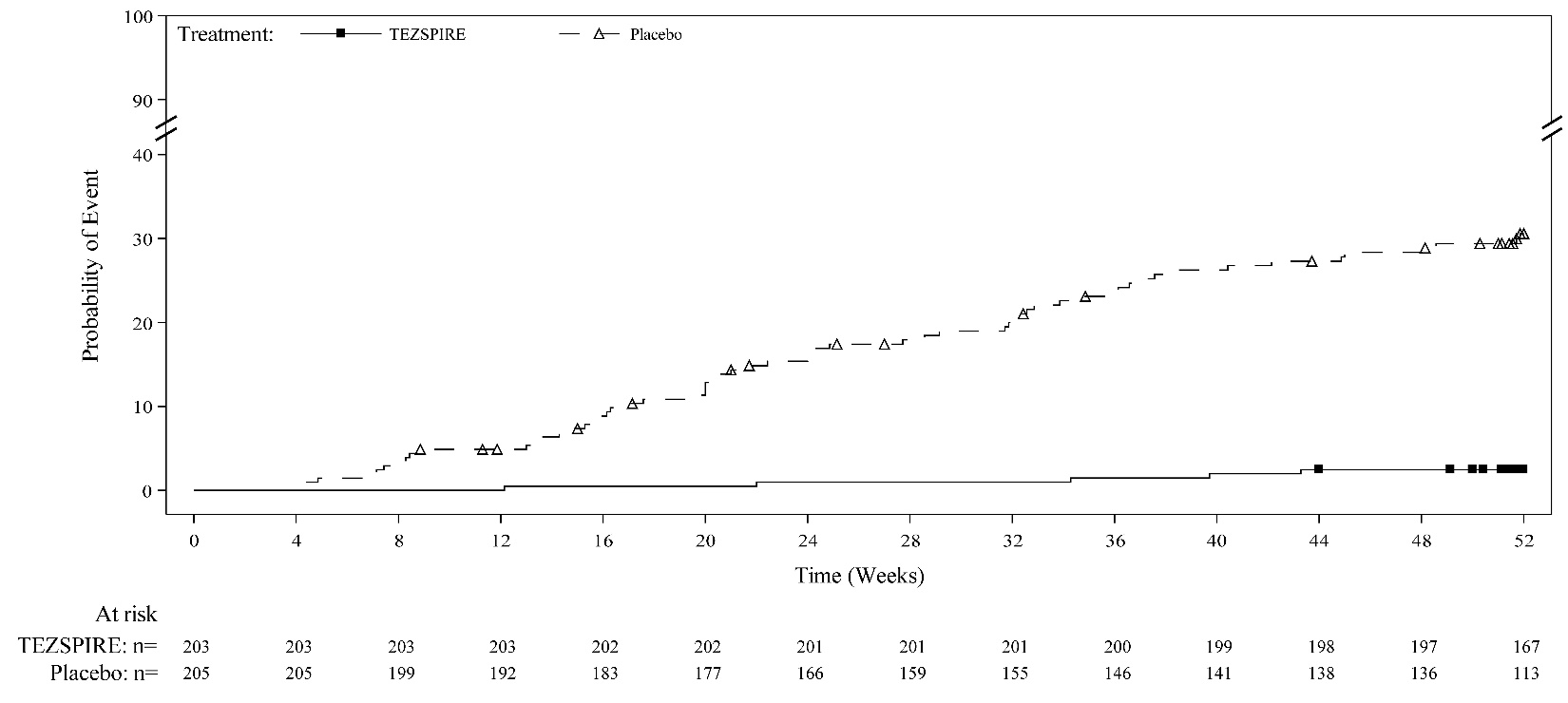
TEZSPIRE significantly reduced the proportion of patients requiring sino-nasal surgery by 98% compared to placebo over 52 weeks (Hazard Ratio: 0.02; 95% CI: 0.00, 0.09) and significantly reduced the proportion of patients requiring systemic corticosteroids for CRSwNP by 88% compared to placebo over 52 weeks (Hazard Ratio: 0.12; 95% CI: 0.04, 0.27).
The loss of smell score was based on a subject’s daily rating of the severity of their worst difficulty with sense of smell over the past 24 hours on a 0 to 3 scale (0=none, 1=mild, 2=moderate, 3=severe). The loss of smell score was calculated every 2 weeks as the bi-weekly mean. TEZSPIRE significantly improved the loss of smell compared to placebo. The LS mean difference for loss of smell at Week 52 in the TEZSPIRE group versus placebo was -1.01 [95% CI: -1.18, -0.83].
The LMK sinus CT scan score evaluated the opacification of each sinus at baseline and Week 52 using a 0 to 2 scale (0=no abnormality; 1=partial opacification, 2=total opacification) deriving a maximum score of 12 per side and a total maximum score of 24 (higher scores indicate more opacification). A significant decrease in the LMK sinus CT scan score was observed. The LS mean difference for LMK sinus CT scan score at Week 52 in the TEZSPIRE group versus placebo was -5.76 [95% CI: -6.45, -5.07].
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
TEZSPIRE (tezepelumab-ekko) injection is a sterile, preservative-free, clear to opalescent, colorless to light yellow solution supplied as a single-dose vial, single-dose pre-filled syringe with a fixed 27-gauge ½ inch needle with a needle cover or single-dose pre-filled pen with a fixed 27-gauge ½ inch needle with a needle cover. The vial, pre-filled syringe and pre-filled pen, including the needle cover and stopper, are not made with natural rubber latex.
TEZSPIRE is available as:
-
Single-Dose Vial: Carton contains one 210 mg/1.91 mL (110 mg/mL) glass vial (NDC 55513‑100‑01) -
Single-Dose Pre-filled Syringe: Carton contains one 210 mg/1.91 mL (110 mg/mL) pre-filled syringe (NDC 55513‑112‑01) -
Single-Dose Pre-filled Pen: Carton contains one 210 mg/1.91 mL (110 mg/mL) pre-filled pen (NDC 55513-123‑01)
Storage and Handling
Store refrigerated between 36°F to 46°F (2°C to 8°C). If necessary, TEZSPIRE may be kept at room temperature between 68°F to 77˚F (20°C to 25°C) for a maximum of 30 days. Do not put back in the refrigerator once TEZSPIRE has reached room temperature. After removal from the refrigerator, TEZSPIRE must be used within 30 days or discarded.
Store TEZSPIRE in original carton to protect from light until time of use.
Do not freeze. Do not shake. Do not expose to heat.
17 PATIENT COUNSELING INFORMATION
Advise the patient and/or caregiver to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Hypersensitivity Reactions
Inform patients that hypersensitivity reactions (e.g., anaphylaxis, rash and allergic conjunctivitis) can occur following administration of TEZSPIRE [see Contraindications (4) and Adverse Reactions (6)]. These reactions can occur within hours of administration, but in some instances have a delayed onset (i.e., days). Instruct patients to contact their healthcare provider if they experience symptoms of an allergic reaction [see Warnings and Precautions (5.1) ].
Not for Acute Symptoms or Deteriorating Disease
Inform patients that TEZSPIRE does not treat acute asthma symptoms or acute exacerbations. Inform patients to seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with TEZSPIRE [see Warnings and Precautions (5.2)].
Risk Associated with Abrupt Reduction of Corticosteroid Dosage
Inform patients to not discontinue systemic or inhaled corticosteroids except under the direct supervision of a healthcare provider. Inform patients that reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy [see Warnings and Precautions (5.3)].
Administration of Vaccines
Instruct patients to inform the healthcare provider that they are taking TEZSPIRE prior to a potential vaccination [see Warnings and Precautions (5.5)].
Proper Storage and Disposal
Advise patients to refrigerate TEZSPIRE at 36°F to 46°F (2°C to 8°C). TEZSPIRE may be kept at room temperature between 68°F to 77˚F (20°C to 25°C) for a maximum of 30 days [see How Supplied/Storage and Handling (16)]. Inform patients and caregivers of the need for proper disposal of the pre-filled pen after use, including the use of a sharps disposal container.
Manufactured by: AstraZeneca AB, Södertälje, Sweden SE-15185
US License No. 2059
At: Amgen Inc., One Amgen Center Drive, Thousand Oaks, CA 91320-1799
Marketed by: Amgen Inc. and AstraZeneca AB
©AstraZeneca and Amgen 2025
TEZSPIRE is a trademark of Amgen Inc. and AstraZeneca.



PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
NDC 55513-100-01 Rx only
TEZSPIRETM
(tezepelumab-ekko)
Injection
210 mg/1.91 mL (110 mg/mL)
For Subcutaneous Injection Only
1 singe-dose vial. Discard unused portion.
AMGEN® AstraZeneca
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
NDC 55513-112-01
TEZSPIRETM (tezepelumab-ekko) Injection
210 mg/1.91 mL (110 mg/mL)
Rx Only
For Subcutaneous Injection Only
Store the pre-filled syringe refrigerated at 36° F to 46° F
(2° C to 8° C) in original carton to protect from light.
DO NOT SHAKE, FREEEZE, OR EXPOSE TO HEAT.
1 Singe-dose pre-filled syringe. Discard unused portion
AMGEN® AstraZeneca
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
NDC 55513-123-01 Rx only
TEZSPIRE®
(tezepelumab-ekko)
Injection
210 mg/1.91 mL (110 mg/mL)
For Subcutaneous Injection Only
Store the pre-filled pen refrigerated at 36°F to 46°F
(2°C to 8°C) in original carton to protect from light.
DO NOT SHAKE FREEZE OR EXPOSE TO HEAT.
1 Single-dose pre-filled pen.
Discard unused portion.
ATTENTION: Follow enclosed “Instructions for Use”
to prepare and deliver your dose.
AMGEN® AstraZeneca
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.