Auvi-Q (epinephrine) injection, solution
1 INDICATIONS AND USAGE
AUVI-Q is indicated for the emergency treatment of type I allergic reactions, including anaphylaxis, in adult and pediatric patients who weigh 7.5 kg or greater.
AUVI-Q is a non-selective alpha and beta-adrenergic receptor agonist indicated for the emergency treatment of type I allergic reactions, including anaphylaxis, in adult and pediatric patients who weigh 7.5 kg or greater. (1)
2 DOSAGE AND ADMINISTRATION
The recommended dosage of AUVI-Q is based on weight. (2.1) Administer AUVI-Q intramuscularly or subcutaneously into the anterolateral aspect of the thigh, through clothing if necessary. (2.2)
Recommended Dosage
In the absence of clinical improvement or if symptoms worsen after the initial treatment, a second dose of AUVI-Q may be administered with a second autoinjector starting 5 minutes after the first dose. (2.1)
- Advise patients when to seek emergency medical assistance for close monitoring of the anaphylactic episode and in the event further treatment is required. (2.1)
- It is recommended that patients are prescribed and have immediate access to two AUVI-Q devices at all times. (2.1)
- See full prescribing information for administration instructions. (2.2)
2.1 Recommended Dosage
The recommended dosage for patients who weigh 7.5 kg or greater is based on weight and the dosage is provided in Table 1. Administer AUVI-Q intramuscularly or subcutaneously into the anterolateral aspect of the thigh.
Table 1. Recommended Dosage of AUVI-Q Based on Patient’s Weight
- Since the doses of epinephrine delivered from AUVI-Q are fixed, use other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
- In the absence of clinical improvement or if symptoms worsen after the initial treatment, a second dose of AUVI-Q may be administered with a second autoinjector starting 5 minutes after the first dose.
- Advise patients when to seek emergency medical assistance for close monitoring of the anaphylactic episode and in the event further treatment is required.
- It is recommended that patients are prescribed and have immediate access to two AUVI-Q devices at all times.
2.2 Administration Instructions
- Each AUVI-Q contains a single dose of epinephrine for single use.
- Visually inspect the epinephrine solution in the viewing window of AUVI-Q for particulate matter, cloudiness, and discoloration prior to administration.
- Instruct caregivers of young children and infants who are prescribed AUVI-Q and who may be uncooperative and kick or move during an injection to hold the child’s leg firmly in place and limit movement prior to and during an injection [see Warnings and Precautions (5.1)].
- Inject AUVI-Q intramuscularly or subcutaneously into the anterolateral aspect of the thigh, through clothing if necessary. Do not inject intravenously, and do not inject into buttocks, digits, hands or feet [see Warnings and Precautions (5.1)].
- If a second dose is needed, administer a new AUVI-Q starting 5 minutes after the first dose. More than two sequential doses of epinephrine should be administered under direct medical supervision. Refer patients and caregivers to the Instructions for Use for detailed administration instructions.
3 DOSAGE FORMS AND STRENGTHS
Injection:
- 0.3 mg (0.3 mg/0.3 mL) epinephrine injection, USP, clear and colorless solution, single-dose prefilled autoinjector
- 0.15 mg (0.15 mg/0.15 mL) epinephrine injection, USP, clear and colorless solution, single-dose prefilled autoinjector
- 0.1 mg (0.1 mg/0.1 mL) epinephrine injection, USP, clear and colorless solution, single-dose prefilled autoinjector
5 WARNINGS AND PRECAUTIONS
- Do not inject intravenously, into buttock, digits, hands, or feet. (5.1)
- Hold the child’s leg firmly in place and limit movement prior to and during injection when administering to young children or infants to minimize the risk of injection-related injury. (5.1)
- Rare cases of serious skin and soft tissue infections have been reported following epinephrine injection. Advise patients to seek medical care if they develop signs or symptoms of infection. (5.2)
- Administer with caution in patients with heart disease; may aggravate angina pectoris or produce ventricular arrhythmias. (5.3)
- May aggravate certain coexisting conditions. (5.3)
- The presence of a sulfite in this product should not deter use. (5.4)
5.1 Injection-Related Complications
AUVI-Q should only be injected into the anterolateral aspect of the thigh [see Dosage and Administration (2.1, 2.2)].
- Do not inject intravenously. Large doses or accidental intravenous injection of epinephrine may result in cerebral hemorrhage due to sharp rise in blood pressure. Rapidly acting vasodilators can counteract the marked pressor effects of epinephrine for this inadvertent administration.
- Do not inject into buttock. Injection into the buttock may not provide effective treatment of anaphylaxis. If AUVI-Q is injected into the buttock, advise the patient to administer a second dose of AUVI-Q into the anterolateral aspect of the thigh and if symptoms worsen or persist, then go immediately to the nearest emergency room for further treatment of anaphylaxis. Additionally, injection into the buttock has been associated with Clostridial infections (gas gangrene). Cleansing with alcohol does not kill bacterial spores, and therefore, does not lower this risk.
- Do not inject into digits, hands or feet. Since epinephrine is a strong vasoconstrictor, accidental injection into the digits, hands or feet may result in loss of blood flow to the affected area and may not provide effective treatment of anaphylaxis. Advise the patient to administer a second dose of AUVI-Q into the anterolateral aspect of the thigh if experiencing anaphylaxis and then go immediately to the nearest emergency room and inform the healthcare provider in the emergency room of the location of the accidental injection. Treatment of such inadvertent administration should consist of vasodilation, in addition to further appropriate treatment of anaphylaxis [see Adverse Reactions (6)].
- Hold leg firmly during injection. To minimize the risk of injection-related injury when administering AUVI-Q to young children or infants, instruct caregivers to hold the child’s leg firmly in place and limit movement prior to and during injection.
5.2 Serious Infections at the Injection Site
Rare cases of serious skin and soft tissue infections, including necrotizing fasciitis and myonecrosis caused by Clostridia (gas gangrene), have been reported at the injection site following epinephrine injection for anaphylaxis. Clostridium spores can be present on the skin and introduced into the deep tissue with subcutaneous or intramuscular injection. While cleansing with alcohol may reduce the presence of bacteria on the skin, alcohol cleansing does not kill Clostridium spores. To decrease the risk of Clostridium infection, do not inject AUVI-Q into the buttock [see Warnings and Precautions (5.1)]. Advise patients to seek medical care if they develop signs or symptoms of infection, such as persistent redness, warmth, swelling, or tenderness, at the epinephrine injection site.
5.3 Risk Associated with Use of Epinephrine in Certain Coexisting Conditions
Some patients may be at greater risk for developing adverse reactions after epinephrine administration. Despite these concerns, the presence of these conditions is not a contraindication to epinephrine administration in an acute, life-threatening situation. Therefore, instruct patients with these conditions, and/or caregivers to the circumstances under which epinephrine should be used.
Administer epinephrine with caution to patients who have heart disease, including patients with cardiac arrhythmias, coronary artery disease, or hypertension. In such patients, or in patients who are on drugs that may sensitize the heart to arrhythmias, epinephrine may precipitate or aggravate angina pectoris as well as produce ventricular arrhythmias [see Drug Interactions (7) and Adverse Reactions (6)].
Epinephrine can temporarily exacerbate the underlying conditions or increase symptoms in patients with the following: hyperthyroidism, Parkinson’s disease, diabetes, renal impairment. Administer epinephrine with caution in patients with these conditions, including elderly patients and pregnant women.
5.4 Allergic Reactions Associated with Sulfite
Epinephrine is the preferred treatment for serious allergic reactions or other emergency situations even though AUVI-Q contains sodium bisulfite, a sulfite that may, in other products, cause allergic-type reactions including anaphylactic symptoms or life-threatening or less severe asthmatic episodes in certain susceptible persons. The alternatives to using epinephrine in a life-threatening situation may not be satisfactory. The presence of a sulfite in AUVI-Q should not deter administration of the drug for treatment of serious allergic or other emergency situations.
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Injection-Related Complications [see Warnings and Precautions (5.1)]
- Serious Infections at the Injection Site [see Warnings and Precautions (5.2)]
- Risks Associated with Use of Epinephrine in Certain Coexisting Conditions [see Warnings and Precautions (5.3)]
- Allergic Reactions Associated with Sulfite [see Warnings and Precautions (5.4)]
Adverse Reactions from Postapproval Use of Epinephrine Products
The following adverse reactions have been identified during postapproval use of epinephrine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Cardiovascular: angina, arrhythmias (including fatal ventricular fibrillation), cerebral hemorrhage, hypertension, pallor, palpitations, tachyarrhythmia, tachycardia, vasoconstriction, ventricular ectopy, and stress cardiomyopathy
Gastrointestinal Disorders: nausea, vomiting
Infections: Clostridial infections (gas gangrene)
Metabolism and Nutrition Disorders: transient hyperglycemia, sweating
Neurological: disorientation, impaired memory, panic, psychomotor agitations, sleepiness, tingling, weakness, hypoesthesia, dizziness, tremor, headache
Psychiatric: anxiety, apprehensiveness, restlessness
Respiratory: respiratory difficulties
Skin and Subcutaneous Tissue Disorders: bruising, bleeding, discoloration, erythema, necrotizing fasciitis, myonecrosis
Adverse reactions to epinephrine include anxiety, apprehensiveness, restlessness, tremor, weakness, dizziness, sweating, palpitations, pallor, nausea and vomiting, headache, and/or respiratory difficulties. (6)
To report SUSPECTED ADVERSE REACTIONS, contact kaleo, Inc. at 1-877-302-8847 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 DRUG INTERACTIONS
- Cardiac glycosides, diuretics, or anti-arrhythmics: observe for development of cardiac arrhythmias. (7.1)
- Tricyclic antidepressants, monoamine oxidase inhibitors, levothyroxine sodium, certain antihistamines, and catechol-O-methyl transferase inhibitors may potentiate effects of epinephrine. (7.2)
- Beta-adrenergic blocking drugs antagonize cardiostimulating and bronchodilating effects of epinephrine. (7.3)
- Alpha-adrenergic blocking drugs antagonize vasoconstricting and hypertensive effects of epinephrine. (7.3)
- Ergot alkaloids may reverse the pressor effects of epinephrine. (7.3)
7.2 Drugs Potentiating Effects of Epinephrine
The effects of epinephrine may be potentiated by tricyclic antidepressants, monoamine oxidase inhibitors, levothyroxine sodium, and certain antihistamines, notably chlorpheniramine, tripelennamine, and diphenhydramine, and catechol-O-methyl transferase (COMT) inhibitors such as entacapone.
7.3 Drugs Antagonizing Effects of Epinephrine
The cardiostimulating and bronchodilating effects of epinephrine are antagonized by beta- adrenergic blocking drugs, such as propranolol.
The vasoconstricting and hypertensive effects of epinephrine are antagonized by alpha- adrenergic blocking drugs, such as phentolamine.
Ergot alkaloids may also reverse the pressor effects of epinephrine.
8 USE IN SPECIFIC POPULATIONS
Elderly patients may be at greater risk of developing adverse reactions. (8.5)
8.1 Pregnancy
Risk Summary
Prolonged experience with epinephrine use in pregnant women over several decades, based on published literature, have not identified a drug associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. There are risks to the mother and fetus associated with anaphylaxis. Epinephrine is first-line treatment of anaphylaxis and should not be delayed (see Clinical Considerations). In animal reproductive studies, epinephrine administered by the subcutaneous route to rabbits, mice, and hamsters during the period of organogenesis was teratogenic at doses 7 times and higher than the maximum recommended human intramuscular and subcutaneous dose on a mg/m2 basis (see Data).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and embryo/fetal risk:
During pregnancy, anaphylaxis can be catastrophic and can lead to hypoxic-ischemic encephalopathy and permanent central nervous system damage or death in the mother and, more commonly, in the fetus or neonate. Treatment of anaphylaxis during pregnancy should not be delayed.
Data
Animal Data:
In an embryofetal development study with rabbits dosed during the period of organogenesis, epinephrine was shown to be teratogenic (including gastroschisis and embryonic lethality) at doses approximately 40 times the maximum recommended intramuscular or subcutaneous dose (on a mg/m2 basis at a maternal subcutaneous dose of 1.2 mg/kg/day for two to three days).
In an embryofetal development study with mice dosed during the period of organogenesis, epinephrine was shown to be teratogenic (including embryonic lethality) at doses approximately 8 times the maximum recommended intramuscular or subcutaneous dose (on a mg/m2 basis at a maternal subcutaneous dose of 1 mg/kg/day for 10 days). These effects were not seen in mice at approximately 4 times the maximum recommended daily intramuscular or subcutaneous dose (on a mg/m2 basis at a subcutaneous maternal dose of 0.5 mg/kg/day for 10 days).
In an embryofetal development study with hamsters dosed during the period of organogenesis from gestation days 7 to 10, epinephrine was shown to be teratogenic at doses approximately 7 times the maximum recommended daily intramuscular or subcutaneous dose (on a mg/m2 basis at a maternal subcutaneous dose of 0.5 mg/kg/day for 4 days).
8.2 Lactation
Risk Summary
There is no information on the presence of epinephrine in human milk, the effects on breastfed infants, or the effects on milk production. However, due to its poor oral bioavailability and short half-life, transfer of epinephrine into breastmilk is expected to be low. Treatment of anaphylaxis in breastfeeding patients should not be delayed.
8.4 Pediatric Use
The safety and effectiveness of AUVI-Q for the emergency treatment of type I allergic reactions, including anaphylaxis have been established in pediatric patients who weigh 7.5 kg or greater. The use of AUVI-Q for this indication is supported by clinical experience. Clinical experience with the use of epinephrine suggests that the adverse reactions seen in pediatric patients are similar in nature and extent to those both expected and reported in adults. Since the doses of epinephrine delivered from AUVI-Q are fixed, use other forms of injectable epinephrine if doses lower than 0.1 mg are deemed necessary.
The safety and effectiveness of AUVI-Q have not been established in pediatric patients who weigh less than 7.5 kg.
8.5 Geriatric Use
Clinical studies of AUVI-Q for emergency treatment of type I allergic reactions, including anaphylaxis, were not conducted to determine whether they respond differently from younger patients. However, other reported clinical experience with use of epinephrine for treatment of anaphylaxis has identified that geriatric patients may be particularly sensitive to the effects of epinephrine. Therefore, these patients may be at greater risk for developing adverse reactions after epinephrine administration [see Overdosage (10)].
10 OVERDOSAGE
Overdosage of epinephrine has been reported to produce extremely elevated arterial pressure, which may result in cerebrovascular hemorrhage, particularly in elderly patients. Overdosage may also result in pulmonary edema because of peripheral vascular constriction together with cardiac stimulation.
Epinephrine overdosage can also cause transient bradycardia followed by tachycardia, which may be accompanied by fatal cardiac arrhythmias; premature ventricular contractions followed by multifocal ventricular tachycardia; atrial tachycardia and occasionally by atrioventricular block; extreme pallor and coldness of the skin; metabolic acidosis; kidney failure.
Epinephrine is rapidly inactivated in the body and treatment following overdosage with epinephrine is primarily supportive. Treatment of epinephrine associated pulmonary edema consists of a rapidly acting alpha-adrenergic blocking drug (such as phentolamine mesylate) and respiratory support. Treatment of epinephrine associated arrhythmias consists of administration of a beta-adrenergic blocking drug (such as propranolol). If necessary, pressor effects may be counteracted by rapidly acting vasodilators or α-adrenergic blocking drugs. If prolonged hypotension follows such measures, it may be necessary to administer another pressor drug.
Consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations.
11 DESCRIPTION
AUVI-Q (epinephrine injection, USP) 0.3 mg, 0.15 mg and 0.1 mg is an autoinjector and a combination product containing drug and device components.
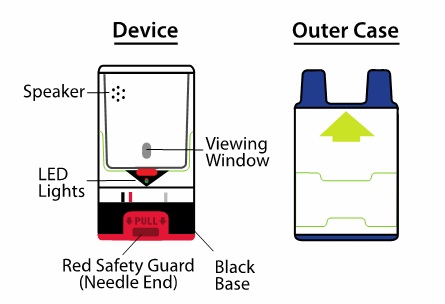
AUVI-Q includes audible (electronic voice instructions, beeps) and visible (LED lights) cues for use. The needle automatically retracts after the injection is complete.
Each AUVI-Q 0.3 mg delivers a single dose of 0.3 mg epinephrine from epinephrine injection, USP (0.3 mL) in a sterile solution.
Each AUVI-Q 0.15 mg delivers a single dose of 0.15 mg epinephrine from epinephrine injection, USP (0.15 mL) in a sterile solution.
Each AUVI-Q 0.1 mg delivers a single dose of 0.1 mg epinephrine from epinephrine injection, USP (0.1 mL) in a sterile solution.
AUVI-Q 0.3 mg, AUVI-Q 0.15 mg and AUVI-Q 0.1 mg each contain 0.76 mL epinephrine solution. 0.3 mL, 0.15 mL and 0.1 mL epinephrine solution is dispensed for AUVI-Q 0.3 mg, AUVI-Q 0.15 mg and AUVI-Q 0.1 mg, respectively, when activated. The remaining solution is not available for future use and should be discarded.
Each 0.3 mL in AUVI-Q 0.3 mg contains 0.3 mg epinephrine, 2.3 mg sodium chloride, 0.45 mg sodium bisulfite, hydrochloric acid to adjust pH, and water for injection. The pH range is 2.2– 5.0.
Each 0.15 mL in AUVI-Q 0.15 mg contains 0.15 mg epinephrine, 1.2 mg sodium chloride, 0.225 mg sodium bisulfite, hydrochloric acid to adjust pH, and water for injection. The pH range is 2.2–5.0.
Each 0.1 mL in AUVI-Q 0.1 mg contains 0.1 mg epinephrine, 0.78 mg sodium chloride, 0.15 mg sodium bisulfite, hydrochloric acid to adjust pH, and water for injection. The pH range is 2.2–5.0.
Epinephrine is a sympathomimetic catecholamine. Chemically, epinephrine is (-)-3,4-Dihydroxy-a-[(methylamino)methyl]benzyl alcohol with the following structure:
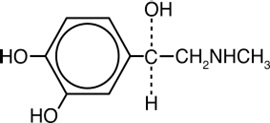
Epinephrine solution deteriorates rapidly on exposure to air or light, turning pink from oxidation to adrenochrome and brown from the formation of melanin.
AUVI-Q is not made with natural rubber latex.
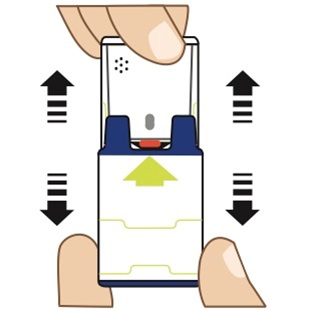
AUVI-Q instructional and safety systems should be thoroughly reviewed with patients and caregivers prior to use [see Patient Counseling Information (17)].
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Epinephrine acts on both alpha and beta-adrenergic receptors.
Through its action on alpha-adrenergic receptors, epinephrine lessens the vasodilation and increased vascular permeability that occurs during anaphylaxis, which can lead to loss of intravascular fluid volume and hypotension.
Through its action on beta-adrenergic receptors, epinephrine causes bronchial smooth muscle relaxation and helps alleviate bronchospasm, wheezing and dyspnea that may occur during anaphylaxis.
Epinephrine also alleviates pruritus, urticaria, and angioedema and may relieve gastrointestinal and genitourinary symptoms associated with anaphylaxis because of its relaxer effects on the smooth muscle of the stomach, intestine, uterus and urinary bladder.
12.2 Pharmacodynamics
When given subcutaneously or intramuscularly, epinephrine has a rapid onset and short duration of action.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies to evaluate the carcinogenic potential of epinephrine have not been conducted.
Epinephrine and other catecholamines have been shown to have mutagenic potential in vitro. Epinephrine was positive in the Salmonella bacterial reverse mutation assay, positive in the mouse lymphoma assay, and negative in the in vivo micronucleus assay. Epinephrine is an oxidative mutagen based on the E. coli WP2 Mutoxitest bacterial reverse mutation assay. This should not prevent the use of epinephrine where indicated [see Indications and Usage (1)].
The potential for epinephrine to impair reproductive performance has not been evaluated, but epinephrine has been shown to decrease implantation in female rabbits dosed subcutaneously with 1.2 mg/kg/day (40-fold the highest human intramuscular or subcutaneous daily dose) during gestation days 3 to 9.
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
AUVI-Q (epinephrine injection) is a clear and colorless solution for intramuscular or subcutaneous use. AUVI-Q is available as an autoinjector as described in Table 2.
Table 2. AUVI-Q Autoinjector Package Configurations and Strengths
Storage and Handling
- Protect from light. Epinephrine is light sensitive and should be stored in the outer case.
- Store at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [See USP Controlled Room Temperature]. Do not freeze.
- Before using, check to make sure the solution in the autoinjector is clear and colorless. Replace the autoinjector if the solution is discolored, cloudy, or contains particles.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Administration and Training
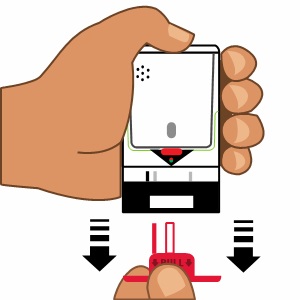
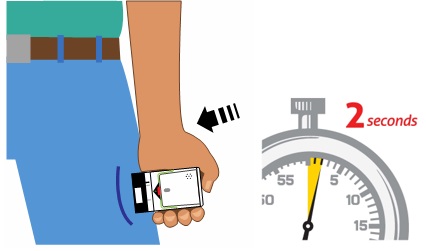
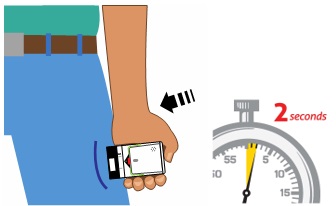
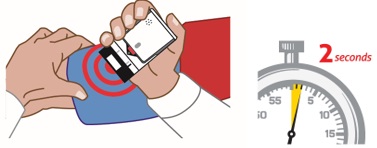
- Instruct patients and/or caregivers in the appropriate use of AUVI-Q. AUVI-Q should be injected into the middle of the outer thigh (through clothing, if necessary). Each device is a single-dose injection.
- Advise patients and/or caregivers when to seek emergency medical care for close monitoring of the type I allergic emergency and in the event that further treatment is required.
- Instruct patients and/or caregivers to inspect the epinephrine solution visually through the viewing window periodically. AUVI-Q should be replaced if the epinephrine solution appears discolored, cloudy, or contains particles.
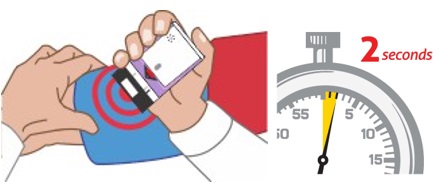
- Instruct caregivers to hold the leg of young children or infants firmly in place and limit movement prior to and during injection [see Warnings and Precautions (5.1)].
- Instruct patients and/or caregivers that the needle will not be visible after the injection and they may not feel the injection when it occurs.
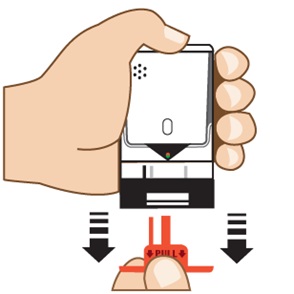
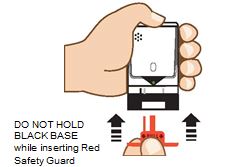
- Instruct patients and/or caregivers that AUVI-Q includes a 2- second countdown after it is activated and then the voice instructions will indicate when the injection has been completed and to seek medical care, if needed. Instruct patients that AUVI-Q’s black base will lock up onto the device housing and the lights will blink red after the injection has been completed. These post-use indicators help patients and/or caregivers know that AUVI-Q has been activated and an epinephrine injection has been administered.
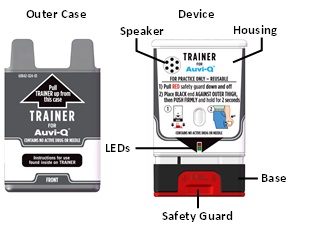
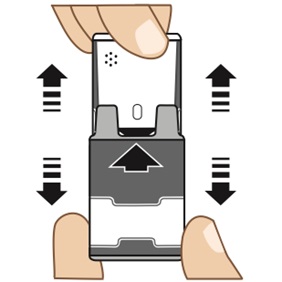
- Instruct patients and/or caregivers to use and practice with the Trainer to familiarize themselves with the use of AUVI-Q in an allergic emergency. The Trainer may be used multiple times.
Injection-Related Complications
Advise patients to seek immediate medical care in the case of accidental injection into the digits, hands, or feet because such an accidental injection to these areas may cause loss of blood flow to the affected area [see Warnings and Precautions (5.1)].
Serious Infections at the Injection Site
Advise patients that rare cases of serious skin and soft tissue infections, including necrotizing fasciitis and myonecrosis caused by Clostridia (gas gangrene), have been reported at the injection site following epinephrine injection for anaphylaxis. Instruct patients to seek medical care if they develop signs or symptoms of infection, such as persistent redness, warmth, swelling, or tenderness, at the epinephrine injection site [see Warnings and Precautions (5.2)].
Risks Associated with Certain Coexisting Conditions
Advise patients with coexisting conditions (cardiac arrhythmia and ischemia, hypertension, pulmonary edema, hyperthyroidism, renal impairment, Parkinson’s disease, diabetes), for increased risks that may be associated with use of epinephrine [see Warnings and Precautions (5.3)].
Storage and Handling
Epinephrine is light sensitive and should be stored in the outer case provided to protect it from light. Instruct patients that AUVI-Q must be used or properly disposed once the red safety guard is removed [see How Supplied/Storage and Handling (16)].
Manufactured for:
kaleo, Inc.
Richmond, VA 23219 USA
This product may be covered by one or more U.S. patents or pending patent applications; see www.kaleo.com for details. KALÉO® and AUVI-Q® are registered trademarks of kaleo, Inc.
© 2025 kaleo, Inc.
*For California Only: This product uses batteries containing Perchlorate Material – special handling may apply. See www.dtsc.ca.gov/hazardouswaste/perchlorate




Storage:
- Store the TRAINER for AUVI-Q at room temperature; the TRAINER for AUVI-Q should not be used at temperatures less than 50°F (10°C) or greater than 104°F (40°C).
- Store the TRAINER for AUVI-Q in its outer case.
- Keep the TRAINER for AUVI-Q away from dirt, chemicals, and water.
Disposal:
The TRAINER for AUVI-Q contains electronics and lithium coin cell batteries, and should be disposed of in the correct manner. Follow your State and local environmental regulations for disposal.
For California Only: This product uses batteries containing Perchlorate Material - special handling may apply. See www.dtsc.ca.gov/hazardouswaste/perchlorate
Manufactured for:
kaleo, Inc.
Richmond, VA 23219 USA
This product may be covered by one or more U.S. patents or pending patent applications; see www.kaleo.com for details. KALÉO® and AUVI-Q® are registered trademarks of kaleo, Inc.
© 2025 kaleo, Inc.
Rev. Apr 2025
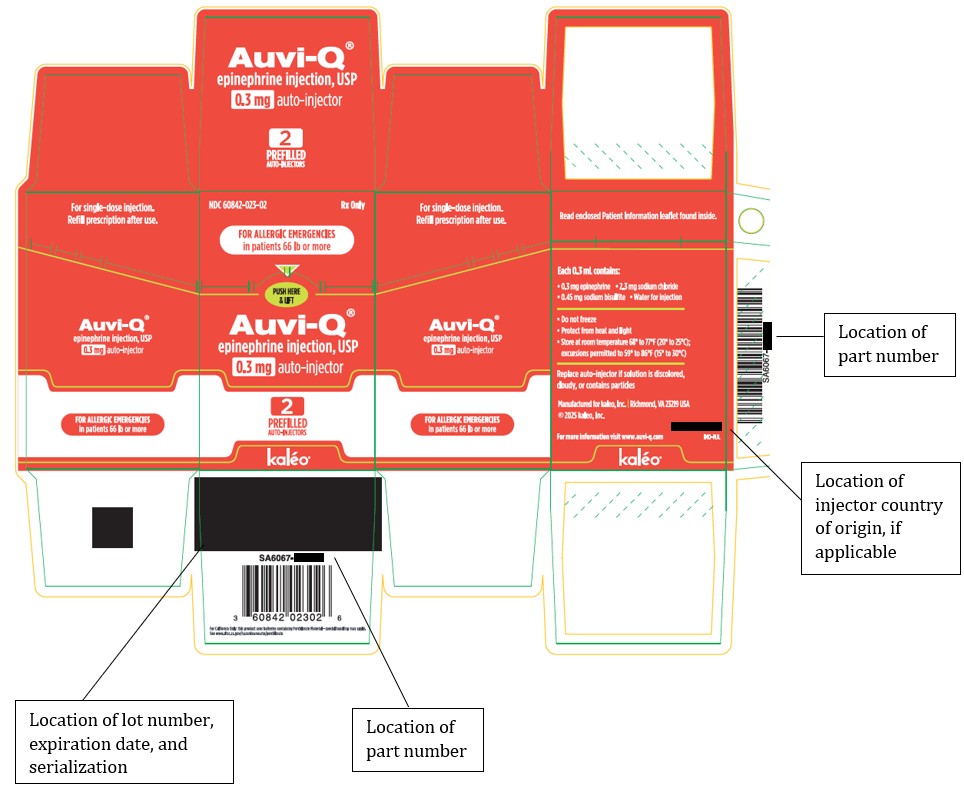
PRINCIPAL DISPLAY PANEL - NDC: 60842-023-02 - 0.3 mg Carton Label
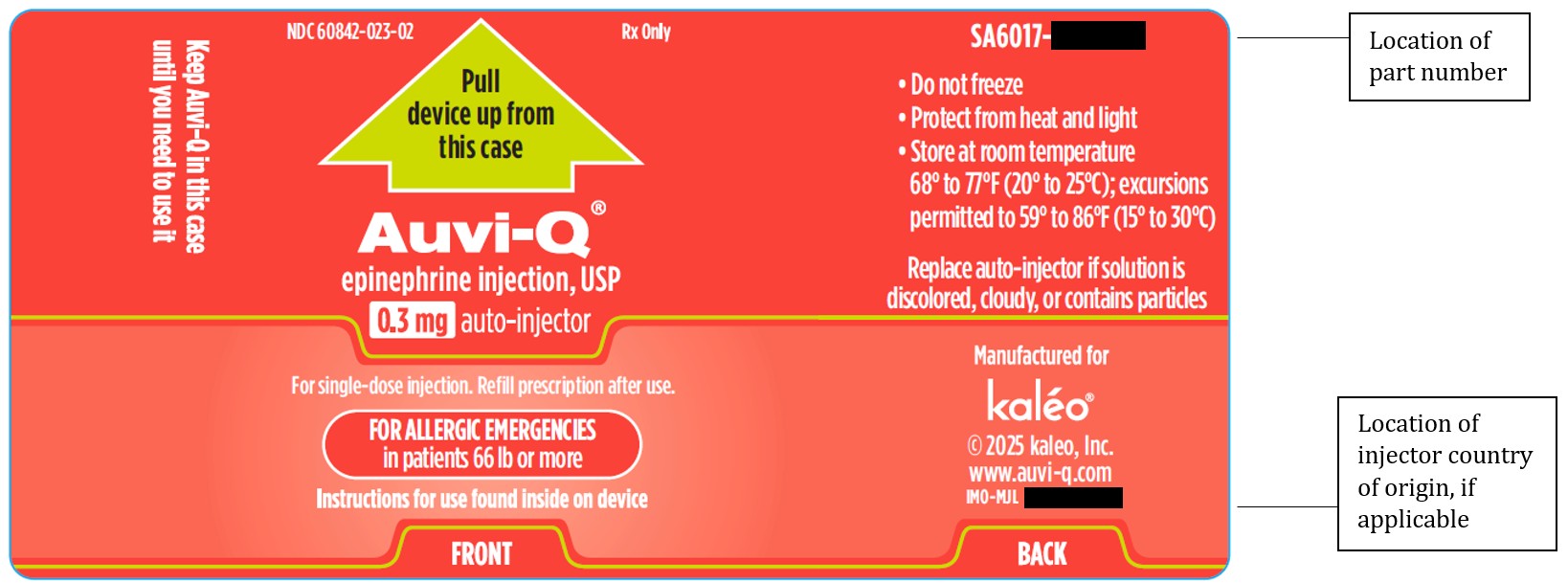
PRINCIPAL DISPLAY PANEL - NDC: 60842-023-02 - 0.3 mg Outer Case Label
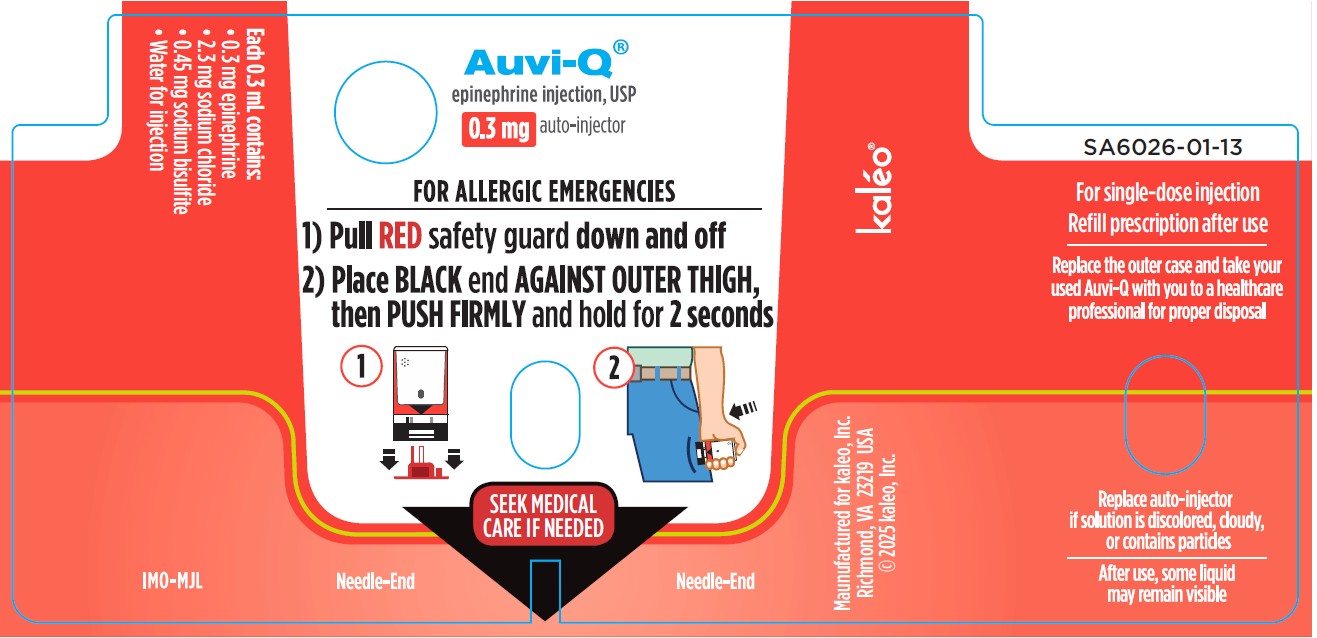
PRINCIPAL DISPLAY PANEL - NDC: 60842-023-02 - 0.3 mg Device Label
PRINCIPAL DISPLAY PANEL - NDC: 60842-022-02 - 0.15 mg Carton Label
PRINCIPAL DISPLAY PANEL - NDC: 60842-022-02 - 0.15 mg Outer Case Label
PRINCIPAL DISPLAY PANEL - NDC: 60842-022-02 - 0.15 mg Device Label
PRINCIPAL DISPLAY PANEL - NDC: 60842-024-01 - Trainer Carton Label (Supplied with 0.3 mg and 0.15 mg Auto-Injectors)

PRINCIPAL DISPLAY PANEL - NDC: 60842-024-01 - Trainer Outer Case Label (Supplied with 0.3 mg and 0.15 mg Auto-Injectors)
PRINCIPAL DISPLAY PANEL - NDC: 60842-024-01 - Trainer Device Label (Supplied with 0.3 mg and 0.15 mg Auto-Injectors)
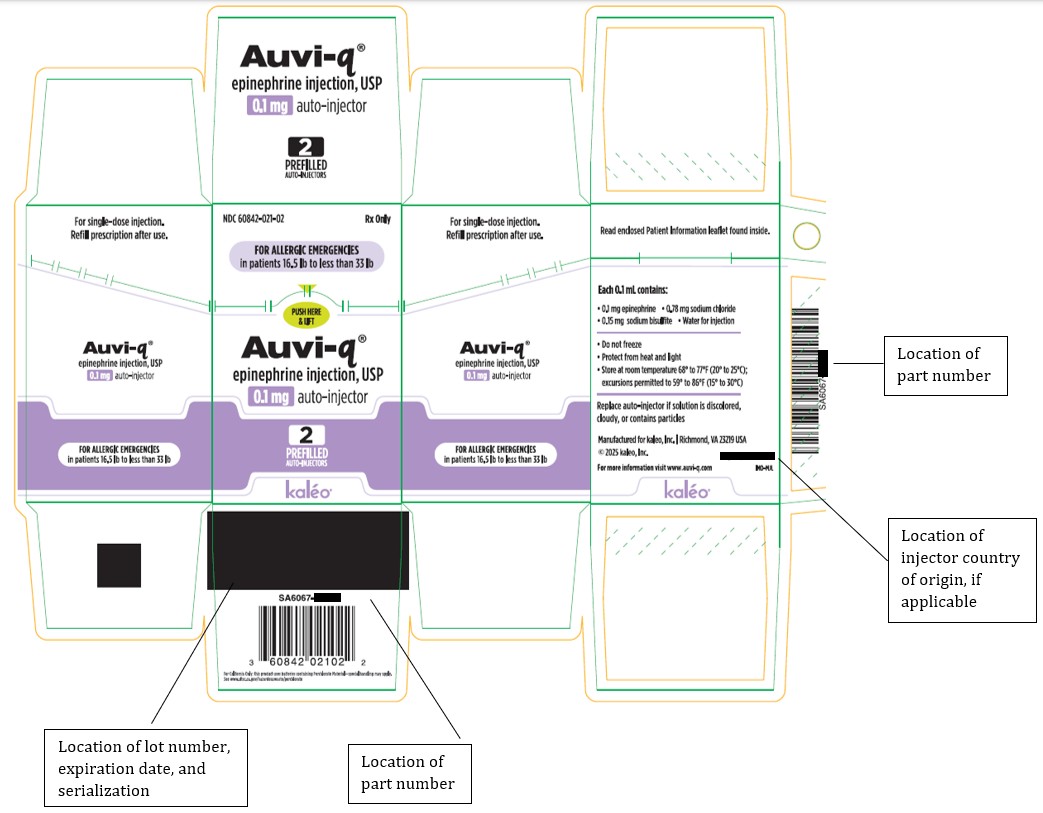
PRINCIPAL DISPLAY PANEL - NDC: 60842-021-02 - 0.1 mg Carton Label
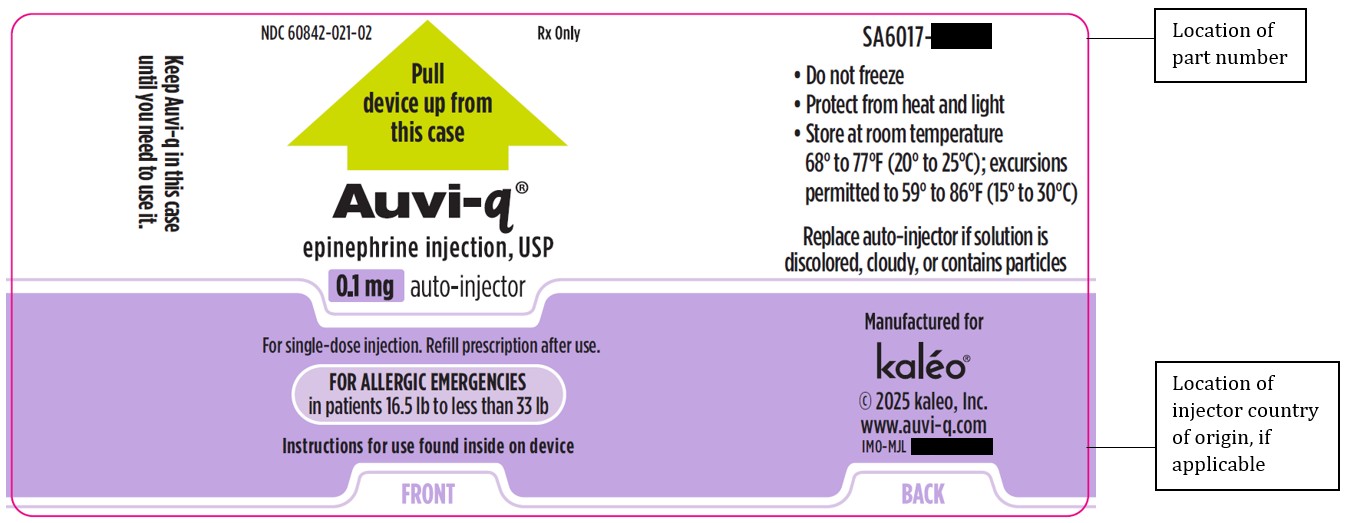
PRINCIPAL DISPLAY PANEL - NDC: 60842-021-02 - 0.1 mg Outer Case Label
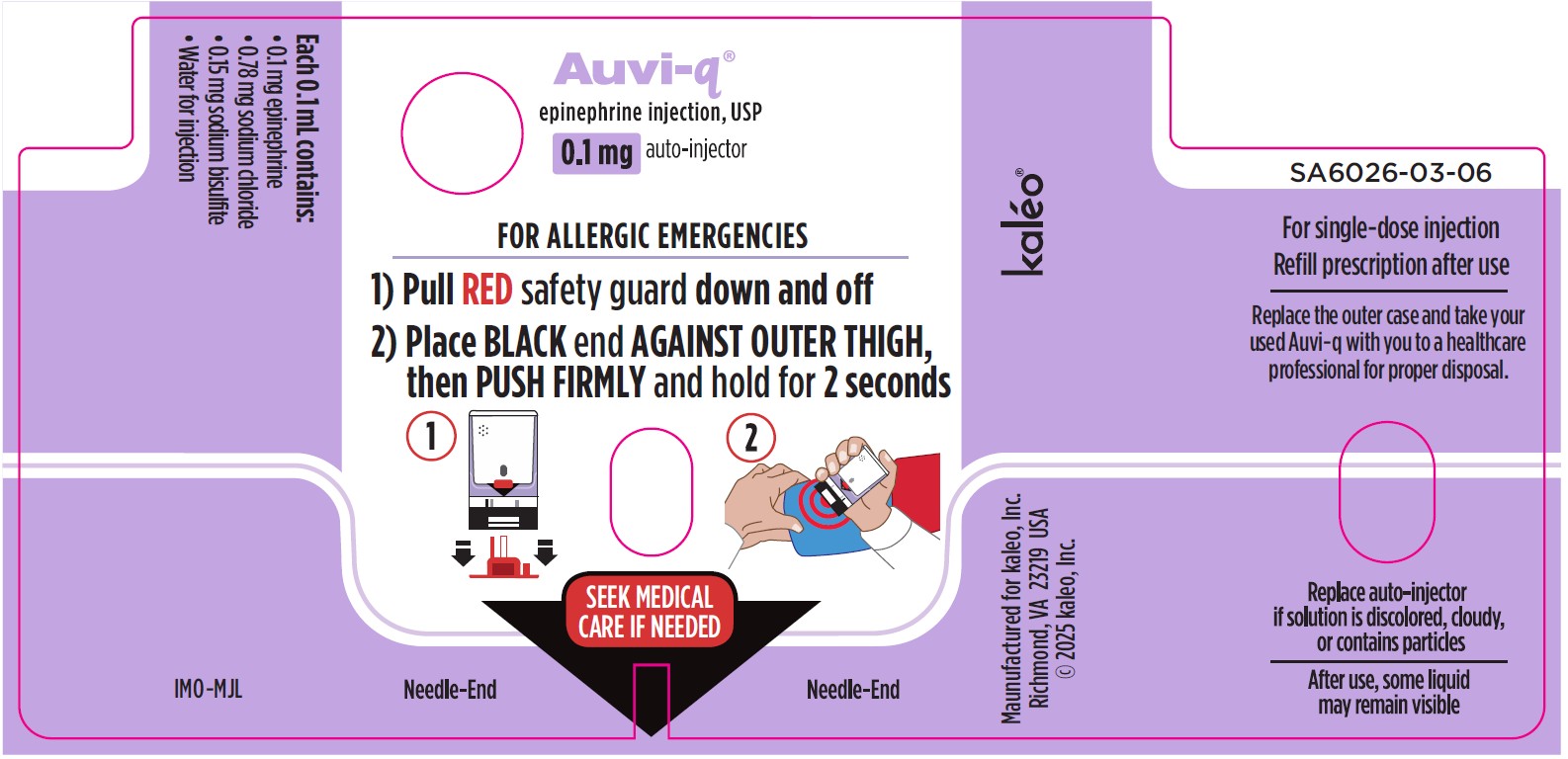
PRINCIPAL DISPLAY PANEL - NDC: 60842-021-02 - 0.1 mg Device Label
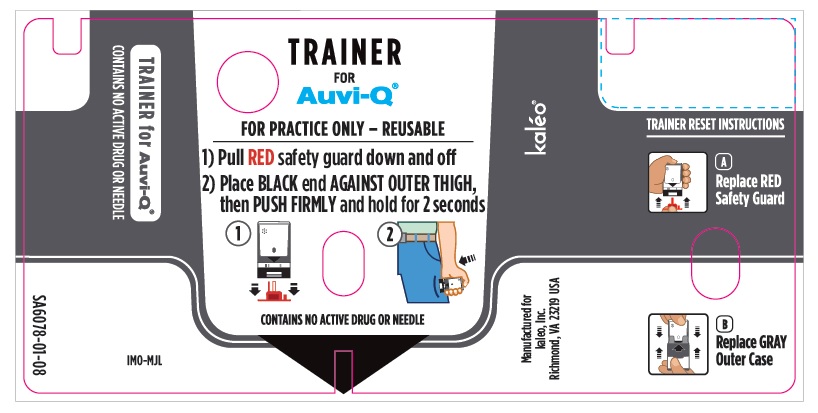
PRINCIPAL DISPLAY PANEL - NDC: 60842-025-01 - Trainer Carton Label (Supplied with 0.1 mg Auto-Injectors)
PRINCIPAL DISPLAY PANEL - NDC: 60842-025-01 - Trainer Outer Case Label (Supplied with 0.1 mg Auto-Injectors)
PRINCIPAL DISPLAY PANEL - NDC: 60842-025-01 - Trainer Device Label (Supplied with 0.1 mg Auto-Injectors)
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.