EVRYSDI (Risdiplam) powder, for solution
1 INDICATIONS AND USAGE
EVRYSDI is indicated for the treatment of spinal muscular atrophy (SMA) in pediatric and adult patients.
EVRYSDI is a survival of motor neuron 2 (SMN2) splicing modifier indicated for the treatment of spinal muscular atrophy (SMA) in pediatric and adult patients. (1)
2 DOSAGE AND ADMINISTRATION
- Administer once daily with or without food per the table below (2.1):
- Swallow EVRYSDI tablet whole with water or dispersed in non-chlorinated drinking water (e.g., filtered water). (2.2)
- Administer EVRYSDI for oral solution with the provided oral syringe. (2.2)
- EVRYSDI for oral solution must be constituted by a healthcare provider prior to dispensing. (2.4)
- See Full Prescribing Information for important preparation and administration instructions. (2.2, 2.4)
2.1 Dosing Information
EVRYSDI is administered orally once daily with or without food at approximately the same time each day. The recommended dosage is determined by age and body weight (see Table 1). EVRYSDI tablets are available for patients prescribed the 5 mg dose.
2.2 Important Administration Instructions
It is recommended that a healthcare provider discuss with the patient or caregiver how to prepare the prescribed daily dose prior to administration of the first dose [see Instructions for Use for EVRYSDI for Oral Solution and EVRYSDI Tablets and Patient Information].
EVRYSDI for Oral Solution
In infants who are breastfed, EVRYSDI for oral solution can be administered before or after breastfeeding. EVRYSDI cannot be mixed with formula or milk.
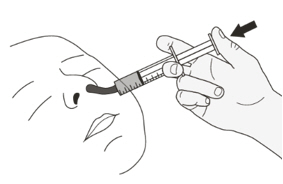
Instruct patients or caregivers to administer the dose using the reusable oral syringe provided.
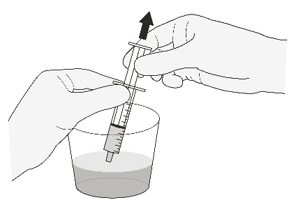
EVRYSDI for oral solution must be taken immediately after it is drawn up into the oral syringe. If EVRYSDI is not taken within 5 minutes, EVRYSDI should be discarded from the oral syringe, and a new dose should be prepared.
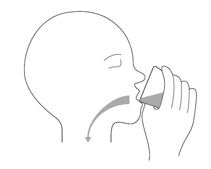
Instruct patients to drink water after taking EVRYSDI for oral solution to ensure the drug has been completely swallowed.
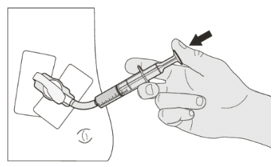
EVRYSDI for oral solution can be administered via a nasogastric or gastrostomy tube. The tube should be flushed with water after delivering EVRYSDI for oral solution [see Instructions for Use].
EVRYSDI Tablets
Swallow EVRYSDI tablets whole with water. Do not chew, cut, or crush the tablets.
Alternatively, the EVRYSDI tablet can also be dispersed in one teaspoon (5 mL) of room temperature non-chlorinated drinking water (e.g., filtered water). EVRYSDI tablets must not be dispersed in any liquid other than non-chlorinated drinking water. Do not expose the prepared dispersion to sunlight. Swirl the small cup gently for up to 3 minutes until fully mixed (though some particles will remain). Administer the dispersed tablet immediately. To ensure no particles are left in the small cup, refill it with at least one tablespoon (15 mL) of non-chlorinated drinking water, swirl, and administer immediately again.
EVRYSDI must be taken immediately after it is dispersed in non-chlorinated drinking water. Discard the prepared dispersion if it is not used within 10 minutes of adding non-chlorinated drinking water.
The dispersed EVRYSDI tablet can be administered via a nasogastric or gastrostomy tube that is 8 French or higher. Flush the tube with the non-chlorinated drinking water [at least one tablespoon (15 mL)] used to rinse the dispersion cup [see Instructions for Use ].
2.3 Missed Dose
If a dose of EVRYSDI is missed, EVRYSDI should be administered as soon as possible if still within 6 hours of the missed dose, and the usual dosing schedule can be resumed on the next day. Otherwise, the missed dose should be skipped, and the next dose should be taken at the regularly scheduled time on the next day.
If a dose is not fully swallowed or vomiting occurs after taking a dose of EVRYSDI, another dose should not be administered to make up for the lost dose. The patient should wait until the next day to take the next dose at the regularly scheduled time.
2.4 Preparation of Powder for Oral Solution by Healthcare Provider
EVRYSDI powder must be constituted to the oral solution by a pharmacist or other healthcare provider prior to dispensing to the patient.
Preparation of the EVRYSDI Oral Solution 0.75 mg/mL
The EVRYSDI "Instructions for Constitution" booklet contains more detailed instructions on the preparation of the oral solution [see Instructions for Constitution].
Caution should be exercised when handling EVRYSDI powder for oral solution. Avoid inhalation and direct contact with skin or mucous membranes with the dry powder and the constituted solution. If such contact occurs, wash thoroughly with soap and water; rinse eyes with water. Wear disposable gloves during the preparation and cleanup procedure.
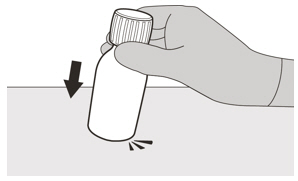
- Gently tap the bottom of the closed glass bottle to loosen the powder.
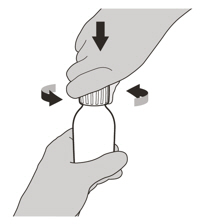
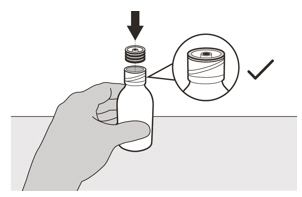
- Remove the cap. Do not throw away the cap.
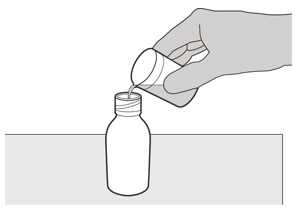
- Carefully pour 79 mL of purified water into the EVRYSDI bottle to yield the 0.75 mg/mL oral solution. Do not mix EVRYSDI with formula or milk.
- Insert the press-in bottle adapter into the bottle opening by pushing it down against the bottle lip. Ensure it is completely pressed against the bottle lip.
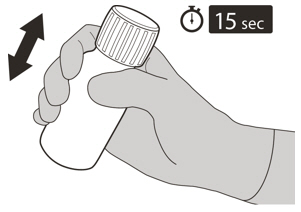
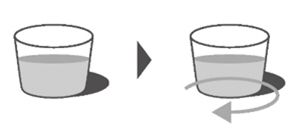
- Re-cap the bottle tightly and shake well for 15 seconds. Wait for 10 minutes. You should have obtained a clear solution. If not, shake well again for another 15 seconds or until you have obtained a clear solution.
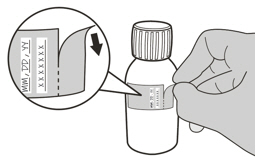
- Write the date of expiration of the constituted oral solution (calculated as 64 days after constitution) and the lot number on the bottle label. Peel off the part of the bottle label that has the expiration date of the powder.
- Put the bottle back in its original carton.
- Select the appropriate oral syringes (1 mL, 6 mL, or 12 mL) based on the patient's dosage and remove the other oral syringes from the carton.
- Dispense with the "Instructions for Use" and FDA-approved patient labeling. Alert patients to read the important handling information described in the Instructions for Use.
Storage
Keep the constituted oral solution of EVRYSDI in the original amber bottle to protect from light. Store in a refrigerator at 2°C to 8°C (36°F to 46°F). Do not freeze. Discard any unused portion 64 days after constitution. Keep the bottle in an upright position with the cap tightly closed. If refrigeration is not available, EVRYSDI can be kept at room temperature up to 40°C (up to 104°F) for a combined total of 5 days. EVRYSDI can be removed from, and returned to, a refrigerator. The total combined time out of refrigeration should not exceed 5 days.
3 DOSAGE FORMS AND STRENGTHS
EVRYSDI for oral solution: 60 mg as a light yellow, pale yellow, yellow, greyish yellow, greenish yellow, or light green powder for constitution. Following constitution, the volume of the greenish yellow to yellow solution is 80 mL, providing 60 mg/80 mL (0.75 mg/mL) risdiplam.
EVRYSDI tablet: 5 mg as a pale yellow film-coated tablet, round and curved, with EVR debossed on one side.
- For Oral Solution: 60 mg of risdiplam as a powder for constitution to provide 0.75 mg/mL solution. (3)
- Tablets: 5 mg
6 ADVERSE REACTIONS
The most common adverse reactions in later-onset SMA (incidence at least 10% of patients treated with EVRYSDI and more frequent than control) were fever, diarrhea, and rash. (6.1)
The most common adverse reactions in infantile-onset SMA were similar to those observed in later-onset SMA patients. Additionally, adverse reactions with an incidence of at least 10% were upper respiratory tract infection, lower respiratory tract infection, constipation, vomiting, and cough. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials including patients with infantile-onset SMA, later-onset SMA, and pre-symptomatic SMA, a total of 491 patients (51% female, 74% Caucasian) were exposed to EVRYSDI for up to a median duration of 48.1 months (range: 0.6 to 63.4 months), with 231 patients receiving treatment for more than 24 months. At the time of first EVRYSDI dose, 90 (18%) patients were 18 years and older, 119 (24%) were 12 years to less than 18 years, 189 (39%) were 2 years to less than 12 years, 67 (14%) 2 months to less than 2 years, and 26 (5%) were less than 2 months.
Clinical Trial in Later-Onset SMA
The safety of EVRYSDI for later-onset SMA is based on data from a randomized, double-blinded, placebo-controlled study (Study 2 Part 2) in patients with SMA Type 2 or 3 (n = 180) [see Clinical Studies (14.2)]. The patient population in Study 2 Part 2 ranged in age from 2 to 25 years at the time of the first dose.
The most common adverse reactions (reported in at least 10% of patients treated with EVRYSDI and at an incidence greater than on placebo) in Study 2 Part 2 were fever, diarrhea, and rash. Table 2 lists the adverse reactions that occurred in at least 5% of patients treated with EVRYSDI and at an incidence ≥ 5% greater than on placebo in Study 2 Part 2.
Clinical Trial in Infantile-Onset SMA
The safety of EVRYSDI therapy for infantile-onset SMA is based on data from an open-label study in 62 patients (Study 1) [see Clinical Studies (14.1)]. The patient population ranged in age from 2 to 7 months at the time of the first EVRYSDI dose (weight range: 4.1 to 10.6 kg).
The most frequent adverse reactions reported in infantile-onset SMA patients treated with EVRYSDI in Study 1 were similar to those observed in later-onset SMA patients in Study 2. Additionally, the following adverse reactions reported in ≥ 10% of patients were: upper respiratory tract infection (including nasopharyngitis, rhinitis), lower respiratory tract infection (including pneumonia, bronchitis), constipation, vomiting, and cough.
Clinical Trial in Pre-Symptomatic SMA
The safety of EVRYSDI therapy for pre-symptomatic SMA is based on data from an open-label, single-arm study in 26 patients (Study 3) [see Clinical Studies (14.3)]. The patient population ranged in age from 16 to 41 days at the time of the first dose (weight range: 3.1 to 5.7 kg). The safety profile of EVRYSDI in pre-symptomatic patients in Study 3 is consistent with the safety profile for symptomatic SMA patients treated with EVRYSDI in clinical trials.
7 DRUG INTERACTIONS
Avoid coadministration with drugs that are substrates of multidrug and toxin extrusion (MATE) transporters. (7.1)
7.1 Effect of EVRYSDI on Substrates of Multidrug and Toxin Extrusion (MATE) Protein Transporters
Based on in vitro data, EVRYSDI may increase plasma concentrations of drugs eliminated via MATE1 or MATE2-K [see Clinical Pharmacology (12.3)], such as metformin. Avoid coadministration of EVRYSDI with MATE substrates. If coadministration cannot be avoided, monitor for drug-related toxicities and consider dosage reduction of the coadministered drug (based on the labeling of that drug) if needed.
8 USE IN SPECIFIC POPULATIONS
Pregnancy: Based on animal data, may cause fetal harm. (8.1)
8.1 Pregnancy
There is a pregnancy exposure registry that monitors pregnancy and fetal/neonatal/infant outcomes in women exposed to EVRYSDI during pregnancy. Physicians are encouraged to register patients and pregnant women are encouraged to register themselves by calling 1-833-760-1098 or visiting https://www.evrysdipregnancyregistry.com.
Risk Summary
There are no adequate data on the developmental risk associated with the use of EVRYSDI in pregnant women. In animal studies, administration of risdiplam during pregnancy or throughout pregnancy and lactation resulted in adverse effects on development (embryofetal mortality, malformations, decreased fetal body weights, and reproductive impairment in offspring) at or above clinically relevant drug exposures [see Data].
The estimated background risk of major birth defects and miscarriage for the indicated populations is unknown. In the U.S. general population, the estimated background risk of major birth defect and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively. Based on animal data, advise pregnant women of the potential risk to the fetus.
Data
Animal Data
Oral administration of risdiplam (0, 1, 3, or 7.5 mg/kg/day) to pregnant rats throughout organogenesis resulted in decreased fetal body weights and increased incidences of fetal structural variations at the highest dose tested, which was not associated with maternal toxicity. The no-effect level for adverse effects on embryofetal development (3 mg/kg/day) was associated with maternal plasma exposure (AUC) approximately 2 times that in humans at the maximum recommended human dose (MRHD) of 5 mg.
Oral administration of risdiplam (0, 1, 4, or 12 mg/kg/day) to pregnant rabbits throughout organogenesis resulted in embryofetal mortality, fetal malformations (hydrocephaly), and structural variations at the highest dose tested, which was associated with maternal toxicity. The no-effect dose for adverse effects on embryofetal development (4 mg/kg/day) was associated with maternal plasma exposure (AUC) approximately 4 times that in humans at the MRHD.
When risdiplam (0, 0.75, 1.5, or 3 mg/kg/day) was orally administered to rats throughout pregnancy and lactation, gestation was prolonged in the dams, and delayed sexual maturation (vaginal opening) and impaired reproductive function (decreased numbers of corpora lutea, implantation sites, and live embryos) were observed in female offspring at the highest dose. The no-effect dose for adverse effects on pre- and postnatal development in rats (1.5 mg/kg/day) was associated with maternal plasma exposure (AUC) similar to that in humans at the MRHD.
8.2 Lactation
Risk Summary
There are no data on the presence of risdiplam in human milk, the effects on the breastfed infant, or the effects on milk production. Risdiplam was excreted in the milk of lactating rats orally administered risdiplam.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for EVRYSDI and any potential adverse effects on the breastfed infant from EVRYSDI or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
Studies of risdiplam in juvenile and adult rats and in monkeys demonstrated adverse effects on the reproductive organs, including germ cells, in males at clinically relevant plasma exposures [see Use in Specific Populations (8.4) and Nonclinical Toxicology (13.1)].
Pregnancy Testing
Pregnancy testing is recommended for females of reproductive potential prior to initiating EVRYSDI [see Use in Specific Populations (8.1)].
Contraception
EVRYSDI may cause embryofetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Female Patients
Advise female patients of reproductive potential to use effective contraception during treatment with EVRYSDI and for at least 1 month after her last dose.
Infertility
Male Patients
Male fertility may be compromised by treatment with EVRYSDI [see Nonclinical Toxicology (13.1)] .
Counsel male patients of reproductive potential receiving EVRYSDI about the potential effects on fertility. Male patients may consider sperm preservation prior to treatment.
8.4 Pediatric Use
The safety and effectiveness of EVRYSDI in pediatric patients (neonates and older) have been established. Use of EVRYSDI for SMA is supported by evidence from adequate and well-controlled studies of EVRYSDI in patients 2 months of age and older with SMA. Use of EVRYSDI for SMA in patients 2 months of age and younger is supported by pharmacokinetic and safety data from pediatric patients 16 days and older, and pharmacokinetic modeling and simulation to identify the dosing regimen [see Clinical Pharmacology (12.3) and Clinical Studies (14)].
Juvenile Animal Toxicity Data
Oral administration of risdiplam (0, 0.75, 1.5, 2.5 mg/kg/day) to young rats from postnatal day (PND) 4 through PND 31 resulted in decreased growth (body weight, tibia length) and delayed sexual maturation in males at the mid and high dose. The skeletal and body weight deficits persisted after cessation of dosing. Ophthalmic changes consisting of vacuoles in the anterior vitreous were seen at the high dose. Decreases in absolute B lymphocyte counts were observed at all doses after cessation of dosing. Decreases in testis and epididymis weights, which correlated with degeneration of the seminiferous epithelium in the testis, occurred at the mid and high doses; the histopathology findings were reversible, but organ weight persisted after cessation of dosing. Impaired female reproductive performance (decreased mating index, fertility index, and conception rate) was observed at the high dose. A no-effect dose for adverse developmental effects on preweaning rats was not identified. The lowest dose tested (0.75 mg/kg/day) was associated with plasma exposures (AUC) lower than that in humans at the maximum recommended human dose (MRHD) of 5 mg/day.
Oral administration of risdiplam (0, 1, 3, or 7.5 mg/kg/day) to young rats from PND 22 through PND 112 produced a marked increase in micronuclei in the bone marrow, male reproductive organ histopathology (degeneration/necrosis of the seminiferous tubule epithelium, oligo/aspermia in the epididymis, spermatic granulomas), and adverse effects on sperm parameters (decreased sperm concentration and motility, increased sperm morphology abnormalities) at the highest dose tested. Increases in T lymphocytes (total, helper, and cytotoxic) were observed at the mid and high doses. The reproductive and immune effects persisted after cessation of dosing. The no-effect dose (1 mg/kg/day) for adverse effects on postweaning juvenile rats was associated with plasma exposures (AUC) lower than that in humans at the MRHD.
8.5 Geriatric Use
Clinical studies of EVRYSDI did not include patients aged 65 years and older to determine whether they respond differently from younger adult patients.
11 DESCRIPTION
EVRYSDI for oral solution and EVRYSDI tablets for oral use contain risdiplam, which is a survival of motor neuron 2 (SMN2)-directed RNA splicing modifier.
The chemical name of risdiplam is 7-(4,7-diazaspiro[2.5]octan-7-yl)-2-(2,8 dimethylimidazo[1,2-b]pyridazin-6-yl)pyrido-4H-[1,2-a]pyrimidin-4-one. Risdiplam has a molecular weight of 401.46 g/mol. Risdiplam demonstrates pH-dependent aqueous solubility; the greatest solubility is at low pH, and solubility decreases with increasing pH. Risdiplam has a pKa1 of 3.78 (base) and pKa2 of 6.62 (base).
The molecular formula of risdiplam is C22H23N7O and the chemical structure is shown below.
EVRYSDI for oral solution is supplied as a powder in an amber glass bottle. Each bottle contains 60 mg of risdiplam. The inactive ingredients of EVRYSDI are: ascorbic acid, disodium edetate dihydrate, isomalt, mannitol, polyethylene glycol 6000, sodium benzoate, strawberry flavor, sucralose, and tartaric acid.
The powder is constituted with purified water to yield 60 mg/80 mL (0.75 mg/mL) of risdiplam after constitution [see Dosage and Administration (2.4)].
Each EVRYSDI tablet contains 5 mg of risdiplam. The inactive ingredients of EVRYSDI tablet are colloidal silicon dioxide, crospovidone, mannitol, microcrystalline cellulose, polyethylene glycol 3350, polyvinyl alcohol, sodium stearyl fumarate, strawberry flavor, talc, tartaric acid, titanium dioxide, and yellow iron oxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Risdiplam is a survival of motor neuron 2 (SMN2) splicing modifier designed to treat patients with spinal muscular atrophy (SMA) caused by mutations in chromosome 5q that lead to SMN protein deficiency. Using in vitro assays and studies in transgenic animal models of SMA, risdiplam was shown to increase exon 7 inclusion in SMN2 messenger ribonucleic acid (mRNA) transcripts and production of full-length SMN protein in the brain.
In vitro and in vivo data indicate that risdiplam may cause alternative splicing of additional genes, including FOXM1 and MADD. FOXM1 and MADD are thought to be involved in cell cycle regulation and apoptosis, respectively, and have been identified as possible contributors to adverse effects seen in animals.
12.2 Pharmacodynamics
In clinical trials for infantile-onset SMA and later-onset SMA patients, EVRYSDI led to an increase in SMN protein with a greater than 2-fold median change from baseline within 4 weeks of treatment initiation across all SMA types studied. The increase was sustained throughout the treatment period (of at least 24 months).
Cardiac Electrophysiology
At the maximum recommended dose, clinically significant QTc interval prolongation was not observed.
12.3 Pharmacokinetics
Pharmacokinetics of EVRYSDI have been characterized in healthy adult subjects and in patients with SMA.
After administration of EVRYSDI as an oral solution, pharmacokinetics of risdiplam were approximately linear between 0.6 and 18 mg in a single-ascending-dose study in healthy adult subjects, and between 0.02 and 0.25 mg/kg once daily in a multiple-ascending-dose study in patients with SMA. Following once-daily oral administration of risdiplam in healthy subjects, approximately 3-fold accumulation of peak plasma concentrations (Cmax) and area under the plasma concentration-time curve (AUC0-24h) was observed. Risdiplam exposures reach steady state 7 to 14 days after once daily administration. EVRYSDI tablet (swallowed whole or dispersed in water) demonstrated comparable bioavailability to EVRYSDI for oral solution in adult healthy volunteers under fasted and fed states.
Absorption
Following oral administration of risdiplam in fasted state, the median time to reach maximum plasma concentration (Tmax) was 3.26 to 4 hours. The Tmax was delayed by up to1 hour in fed state compared to that under fasted state.
Effect of Food
Food (high-fat, high calorie breakfast) had no relevant effect on the exposure of risdiplam. In the clinical efficacy studies (Study 1 and Study 2), risdiplam was administered with a morning meal or after breastfeeding.
Distribution
The apparent volume of distribution at steady state is 190.4 L for a 31.3 kg patient.
Risdiplam is predominantly bound to serum albumin, without any binding to alpha-1 acid glycoprotein, with a free fraction of 11%.
Elimination
The apparent clearance (CL/F) of risdiplam is 2.45 L/h for a 31.3 kg patient.
The terminal elimination half-life of risdiplam was approximately 50 hours in healthy adults.
Metabolism
Risdiplam is primarily metabolized by flavin monooxygenase 1 and 3 (FMO1 and FMO3) and also by CYPs 1A1, 2J2, 3A4, and 3A7.
Parent drug was the major component found in plasma, accounting for 83% of drug-related material in circulation. The pharmacologically-inactive metabolite M1 was identified as the major circulating metabolite.
Excretion
Following a dose of 18 mg, approximately 53% of the dose (14% unchanged risdiplam) was excreted in the feces and 28% in urine (8% unchanged risdiplam).
Specific Populations
There were no clinically significant differences in the pharmacokinetics of EVRYSDI based on race or gender. Renal impairment is not expected to alter the exposures to risdiplam.
The impact of geriatric age on the pharmacokinetics of EVRYSDI has not been studied.
Hepatic Impairment
The pharmacokinetics and safety of risdiplam have been studied in subjects with mild or moderate hepatic impairment (as defined by Child-Pugh class A and B, respectively, n = 8 each) compared to subjects with normal hepatic function (n = 10). Following the administration of 5 mg EVRYSDI, the AUCinf and Cmax of risdiplam were approximately 20% and 5% lower, respectively, in subjects with mild hepatic impairment and were approximately 8% and 20% higher, respectively, in subjects with moderate hepatic impairment, versus matched healthy control subjects. The magnitude of these changes is not considered to be clinically meaningful. The pharmacokinetics and safety in patients with severe hepatic impairment (Child-Pugh class C) have not been studied.
Pediatric Patients
Body weight and age were found to have significant effect on the pharmacokinetics of risdiplam. The estimated exposure (mean AUC0-24h) in pre-symptomatic infants at the age of 1 to 2 months was 2090 ng.h/mL at the recommended dose of 0.15 mg/kg once daily. The estimated exposure for infantile-onset SMA patients (age 2 to 7 months at enrollment) at the recommended dose of 0.2 mg/kg once daily was 1930 ng.h/mL. The estimated exposure for later-onset SMA patients (2 to 25 years old at enrollment) at the recommended dose was 2070 ng.h/mL (0.25 mg/kg once daily for patients with a body weight < 20 kg and 5 mg once daily for patients with a body weight ≥ 20 kg).
No data on risdiplam pharmacokinetics are available in patients less than 16 days of age [see Use in Specific Populations (8.4)].
Drug Interaction Studies
Effect of Other Drugs on EVRYSDI
Coadministration of 200 mg itraconazole (a strong CYP3A inhibitor) twice daily with a single 6 mg oral dose of risdiplam did not have a clinically relevant effect on the pharmacokinetics of risdiplam (11% increase in AUC and 9% decrease in Cmax).
Risdiplam is a weak substrate of human MDR-1 and breast cancer resistant protein (BCRP) transporters in vitro. Human MDR-1 or BCRP inhibitors are not expected to result in a clinically significant increase of risdiplam concentrations.
The effect of omeprazole (an acid-reducing agent/proton pump inhibitor) on risdiplam pharmacokinetics was investigated in healthy subjects. No clinically significant difference was observed in the pharmacokinetics of risdiplam administered as a tablet when used concomitantly with omeprazole. Based on these results, no clinically significant differences are expected with other acid-reducing agents, including H2-receptor antagonists and antacids.
Effect of EVRYSDI on Other Drugs
Risdiplam and its major circulating metabolite M1 did not induce CYP1A2, 2B6, 2C8, 2C9, 2C19, or 3A4 in vitro. Risdiplam and M1 did not inhibit (reversible or time-dependent inhibition) any of the CYP enzymes tested (CYP1A2, 2B6, 2C8, 2C9, 2C19, 2D6), with the exception of CYP3A in vitro.
EVRYSDI is a weak inhibitor of CYP3A. In healthy adult subjects, administration of EVRYSDI once daily for 2 weeks slightly increased the exposure of midazolam, a sensitive CYP3A substrate (AUC 11%; Cmax 16%); this increase is not considered clinically relevant. Based on physiologically-based pharmacokinetic (PBPK) modeling, a similar increase is expected in children and infants as young as 2 months of age.
In vitro studies have shown that risdiplam and its major metabolite are not significant inhibitors of human MDR1, organic anion-transporting polypeptide (OATP) 1B1, OATP1B3, organic anion transporter 1 and 3 (OAT 1 and 3) transporters, and human organic cation transporter 2 (OCT2), at clinically relevant concentrations. Risdiplam and its metabolite are, however, in vitro inhibitors of the multidrug and toxin extrusion (MATE) 1 and MATE2-K transporters [see Drug Interactions (7.1)].
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Risdiplam was not carcinogenic in Tg.rasH2 mice when administered at oral doses of up to 9 mg/kg/day for 26 weeks.
In a 2-year carcinogenicity study in rats, oral administration of risdiplam (0, 0.3, 1, or 3 mg/kg/day) resulted in increased incidences of preputial gland squamous cell carcinomas in males and combined thyroid follicular cell adenomas and carcinomas in females at the highest dose tested. The higher dose not associated with an increase in tumors (1 mg/kg/day) was associated with plasma drug exposures (AUC) similar to that in humans at the maximum recommended human dose (MRHD) of 5 mg/day.
Mutagenesis
Risdiplam was negative in an in vitro Ames assay. In an in vivo combined bone marrow micronucleus and comet assay in rat, risdiplam was clastogenic, as evidenced by an increase in micronuclei in bone marrow, but was negative in the comet assay. A pronounced increase in bone marrow micronuclei was also observed in toxicity studies in adult and juvenile rats [see Use in Specific Populations (8.4)].
Impairment of Fertility
Oral administration of risdiplam to rats for 4 (0, 1, 3, or 9 mg/kg/day) or 26 (0, 1, 3, or 7.5 mg/kg/day) weeks resulted in histopathological effects in the testis (degenerated spermatocytes, degeneration/atrophy of the seminiferous tubules) and epididymis (degeneration/necrosis of ductular epithelium) at the mid and/or high doses. At the high dose in the 26-week study, the testicular lesions persisted to the end of the recovery period, which corresponds, in rat, to approximately one spermatogenic cycle. The no-effect dose for adverse reproductive system effects in adult male rats (1 mg/kg/day) was associated with plasma drug exposures (AUC) similar to that in humans at the maximum recommended human dose (MRHD) of 5 mg/day.
Adverse effects of risdiplam on the testis could not be fully evaluated in the monkey because the majority of monkeys tested were sexually immature. However, oral administration of risdiplam (0, 2, 4, or 6 mg/kg/day) for 2 weeks resulted in histopathological changes in the testis (increases in multinucleate cells, germ cell degeneration) at the highest dose. At the no-effect dose for testicular toxicity in monkeys, plasma exposures were approximately 3 times that in humans at the MRHD.
Oral administration of risdiplam to postweaning juvenile rats resulted in male reproductive toxicity (degeneration/necrosis of the testis seminiferous epithelium with associated oligo/aspermia in the epididymis and abnormal sperm parameters). The no-effect dose for adverse reproductive effects in postweaning male juvenile rats was associated with plasma exposures approximately 4 times that in humans at the MRHD [see Use in Specific Populations (8.4)].
13.2 Animal Toxicology and/or Pharmacology
Retinal toxicity
Risdiplam-induced functional and structural retinal abnormalities were seen in animal studies. In a 39-week toxicity study in monkeys, oral administration of risdiplam (0, 1.5, 3, or 7.5/5 mg/kg/day; high dose lowered after 4 weeks) produced functional abnormalities on the electroretinogram (ERG) in all mid- and high-dose animals at the earliest examination time (Week 20). These findings were associated with retinal degeneration, detected by optical coherence tomography (OCT), on Week 22, the first examination time. The retinal degeneration, with peripheral photoreceptor loss, was irreversible. A no-effect dose for the retinal findings (1.5 mg/kg/day) was associated with plasma exposures (AUC) similar to that in humans at the maximum recommended human dose (MRHD) of 5 mg.
Effect on Epithelial Tissues
Oral administration of risdiplam to rats and monkeys resulted in histopathological changes in epithelium of the gastrointestinal (GI) tract (apoptosis/single cell necrosis), lamina propria (vacuolation), the exocrine pancreas (single cell necrosis), the skin, tongue, and larynx (parakeratosis/hyperplasia/degeneration) with associated inflammation. The skin and GI epithelial effects were reversible. The no-effect doses for effects on epithelial tissues in rats and monkeys were associated with plasma exposures (AUC) similar to that in humans at the MRHD.
14 CLINICAL STUDIES
The efficacy of EVRYSDI for the treatment of patients with infantile-onset, later-onset, and pre-symptomatic SMA was evaluated in three clinical studies, Study 1 (NCT02913482) and Study 2 (NCT02908685), and Study 3 (NCT03779334), respectively.
The overall findings of these studies support the effectiveness of EVRYSDI in SMA pediatric and adult patients and appear to support the early initiation of treatment with EVRYSDI.
14.1 Infantile-Onset SMA
Study 1 was an open-label, 2-part study to investigate the efficacy, safety, pharmacokinetics, and pharmacodynamics of EVRYSDI for oral solution in patients with Type 1 SMA (symptom onset between 28 days and 3 months of age). All patients had genetic confirmation of homozygous deletion or compound heterozygosity predictive of loss of function of the SMN1 gene, and two SMN2 gene copies.
Part 1 of Study 1 was designed as a dose-finding study. Part 2 of Study 1 assessed the safety and efficacy of EVRYSDI at 0.20 mg/kg, the recommended dose determined in Part 1 [see Dosage and Administration (2.4)]. Patients from Part 1 did not take part in Part 2.
A total of 62 patients with symptomatic Type 1 SMA were enrolled in FIREFISH Part 1 (n = 21) and Part 2 (n = 41), of which 58 patients received the recommended dosage [see Dosage and Administration (2.1)]. The median age of onset of clinical signs and symptoms was 1.5 months (range: 0.9 to 3.0 months). The median age at enrollment was 5.6 months (range: 2.2 to 6.9 months), and the median time between onset of symptoms and the first dose was 3.7 months (range 1.0 to 6.0 months). Of these patients, 60% were female, 57% were Caucasian, and 29% were Asian. The demographics and baseline disease characteristics were comparable between Part 1 and Part 2 of the study.
Effectiveness was established based on the ability to sit without support for at least 5 seconds (as measured by Item 22 of the Bayley Scales of Infant and Toddler Development – Third Edition (BSID-III) gross motor scale) and on the basis of survival without permanent ventilation. Permanent ventilation was defined as requiring a tracheostomy or more than 21 consecutive days of either non-invasive ventilation (≥ 16 hours per day) or intubation, in the absence of an acute reversible event.
The primary endpoint was the proportion of patients with the ability to sit without support for at least 5 seconds (BSID-III gross motor scale, Item 22) after 12 months of treatment in Part 2; 29% of patients (n = 12/41) achieved this milestone.
Other efficacy endpoints of EVRYSDI-treated patients in Study 1 (pooled Part 1 and Part 2) are shown in Table 3.
At Month 24, 40% (23/58) of patients who received the recommended dose achieved sitting without support for 30 seconds (BSID-III, Item 26). In addition at Month 24, patients continued to achieve additional motor milestones; 28% (16/58) of patients achieved a standing measure (16% [9/58] supporting weight and 12% [7/58] standing with support), as measured by Section 2 of the Hammersmith Infant Neurological Examination (HINE-2) which assesses motor milestones.
The proportion of patients alive without permanent ventilation (event-free survival) was 84% for all patients at Month 24 (Table 3). Out of 62 patients, 6 infants died (4 within the first 3 months following study enrollment) and one additional patient withdrew from treatment and died 3.5 months later. Four patients required permanent ventilation by Month 24. These results indicate a clinically meaningful deviation from the natural history of untreated infantile-onset SMA. As described in the natural history of untreated infantile-onset SMA, patients would not be expected to attain the ability to sit independently, and no more than 25% of these patients would be expected to survive without permanent ventilation beyond 14 months of age.
14.2 Later-Onset SMA
Study 2 was a 2-part, multicenter trial to investigate the efficacy, safety, pharmacokinetics, and pharmacodynamics of EVRYSDI for oral solution in patients diagnosed with SMA Type 2 or Type 3. Part 1 of Study 2 was dose-finding and exploratory in 51 patients (14% ambulatory). Part 2 was randomized, double-blind, placebo-controlled, and is described below.
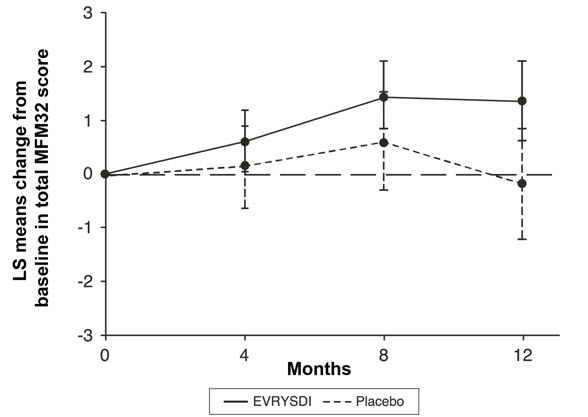
The primary endpoint in Study 2 Part 2 was the change from baseline to Month 12 in the Motor Function Measure 32 (MFM32) score. A key secondary endpoint was the proportion of patients with a 3-point or greater change from baseline to Month 12 in the MFM32 total score. The MFM32 measures motor function abilities that relate to daily functions. The total MFM32 score is expressed as a percentage (range: 0 to 100) of the maximum possible score, with higher scores indicating greater motor function. Another key secondary endpoint was the Revised Upper Limb Module (RULM). The RULM is a tool used to assess motor performance of the upper limb in SMA patients. It tests proximal and distal motor functions of the arm. The total score ranges from 0 (all the items cannot be performed) to 37 (all the activities are achieved fully without any compensatory maneuvers).
Study 2 Part 2 enrolled 180 non-ambulatory patients with Type 2 (71%) or Type 3 (29%) SMA. Patients were randomized 2:1 to receive EVRYSDI at the recommended dosage [see Dosage and Administration (2.1)] or placebo. Randomization was stratified by age group (2 to 5, 6 to 11, 12 to 17, or 18 to 25 years of age).
The median age of patients at the start of treatment was 9.0 years (range: 2 to 25), and the median time between onset of initial SMA symptoms and first treatment was 102.6 months (range: 1 to 275). Of the 180 patients included in the trial, 51% were female, 67% were Caucasian, and 19% were Asian. At baseline, 67% of patients had scoliosis (32% of them with severe scoliosis). Patients had a mean baseline MFM32 score of 46.1, and RULM score of 20.1. Overall baseline demographic characteristics were reasonably balanced between the treatment groups (EVRYSDI and placebo), with the exception of scoliosis (63% in the EVRYSDI arm vs. 73% in the placebo group).
The primary analysis on the change from baseline in MFM32 total score at Month 12 showed a clinically meaningful and statistically significant difference between patients treated with EVRYSDI and placebo. The results of the primary analysis and key secondary endpoints are shown in Table 4 and Figure 1.
14.3 Pre-Symptomatic SMA
Study 3 was an open-label, single-arm, multicenter clinical study to investigate the efficacy, safety, pharmacokinetics, and pharmacodynamics of EVRYSDI in infants up to 6 weeks of age (at first dose) who have been genetically diagnosed with SMA but do not yet present with symptoms.
The efficacy in pre-symptomatic SMA patients was evaluated at Month 12 in 26 patients treated with EVRYSDI in Study 3: 8 patients had 2 copies of the SMN2 gene, 13 patients had 3 copies, and 5 patients had 4 or more copies. The median age of these patients at first dose was 25 days (range: 16 to 41), 62% were female, and 85% were Caucasian. The primary efficacy population (N = 5) included patients with 2 SMN2 copies and a baseline CMAP amplitude ≥1.5 mV.
The primary efficacy endpoint was the proportion of patients with the ability to sit without support for at least 5 seconds (BSID-III gross motor scale, Item 22) at Month 12. This milestone was achieved by 80% (4/5) of patients in the primary efficacy population. This milestone was also achieved by 87.5% (7/8) of all patients with 2 copies of SMN2 and 96.2% (25/26) of patients in the full treated population.
At Month 12, 80.8% (21/26) of patients in the full treated population achieved sitting without support for 30 seconds (BSID-III, Item 26). Of the 26 patients treated with EVRYSDI, 25 patients had motor milestones measured by the HINE-2 at Month 12. Of these, 24 (96%) achieved sitting (23 patients could pivot/rotate and 1 achieved stable sit); 21 (84%) could stand (13 patients could stand unaided and 8 could stand with support); and 12 (48%) could walk independently. Seven patients were not tested for walking at Month 12. All 26 patients were alive at 12 months without permanent ventilation.
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 EVRYSDI for Oral Solution
How Supplied
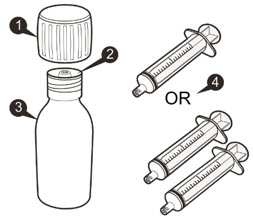
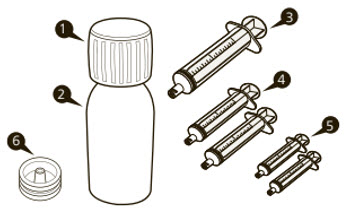
Each amber glass bottle of EVRYSDI for oral solution is packaged with a bottle adapter, two 1 mL reusable oral syringes, two 6 mL reusable oral syringes, and one 12 mL reusable oral syringe. EVRYSDI for oral solution is a light yellow, pale yellow, yellow, greyish yellow, greenish yellow, or light green powder. Each bottle contains 60 mg of risdiplam (NDC 50242-175-07).
Storage and Handling
Store the dry powder at 20°C to 25°C (68°F to 77°F), excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP controlled room temperature]. Keep in the original carton.
Keep the constituted oral solution of EVRYSDI in the original amber bottle to protect from light. Store in a refrigerator at 2°C to 8°C (36°F to 46°F) [see Dosage and Administration (2.4)].
16.2 EVRYSDI Tablets
How Supplied
Pale yellow film-coated tablet, round and curved, with EVR debossed on one side; available in HDPE bottles of 30 tablets with a child-resistant cap (NDC 50242-202-01).
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature]. Keep in the original bottle. Keep the bottle tightly closed in order to protect from moisture.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Pregnancy and Fetal Risk
Inform pregnant women and women of reproductive potential that, based on animal studies, EVRYSDI may cause fetal harm [see Use in Specific Populations (8.1)].
Discuss with women of childbearing age whether they are pregnant, might be pregnant, or are trying to become pregnant.
Advise women of childbearing potential to use effective contraception during treatment with EVRYSDI and for at least 1 month after stopping EVRYSDI.
Advise a female patient to immediately inform the prescriber if she is pregnant or planning to become pregnant [see Use in Specific Populations (8.3)].
Pregnancy Registry
Encourage patients to enroll in the EVRYSDI Pregnancy Registry if they become pregnant while taking EVRYSDI [see Use in Specific Populations (8.1)].
Potential Effects on Male Fertility
Advise male patients that their fertility may be compromised while on treatment with EVRYSDI [see Use in Specific Populations (8.3)].
Instructions for Preparation of Oral Solution
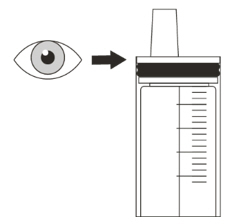
Advise patients/caregivers to ensure that EVRYSDI oral solution is in liquid form when received from the pharmacy.
Instruct patients/caregivers to take EVRYSDI oral solution with or without food or before or after breastfeeding at approximately the same time each day. However, instruct caregivers not to mix EVRYSDI with formula or milk.
Instruct patients/caregivers to take EVRYSDI oral solution immediately after it is drawn up into the reusable oral syringe [see Dosage and Administration (2.2)].
Instructions for EVRYSDI Tablets
Advise patients/caregivers to swallow EVRYSDI tablets whole with water. Do not chew, cut, or crush the tablets.
Alternatively, the tablet can be dispersed in one teaspoon (5 mL) of room temperature non-chlorinated drinking water (e.g., filtered water) and taken immediately. EVRYSDI tablets must not be dispersed in any liquid other than non-chlorinated drinking water. Instruct the patient/caregivers that the dispersion must be administered within 10 minutes of adding non-chlorinated drinking water, or it must be discarded [see Dosage and Administration (2.2)].
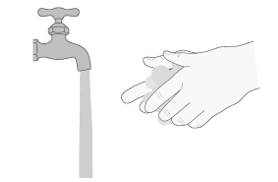
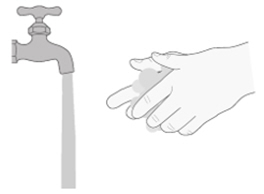
Advise patients/caregivers to wash their hands before and after preparing or taking EVRYSDI tablets.
Advise patients/caregivers to avoid getting the dispersed tablet on their skin or in their eyes. Advise patients/caregivers to wash the area with soap and water if the dispersed tablet gets on the skin. Advise patients/caregivers to rinse their eyes with water if the dispersed tablet gets in the eyes.
Advise patients/caregivers to use a dry paper towel to dry the area if the dispersion is spilled and then clean with soap and water. Advise patients/caregivers to throw the paper towel away in the trash and wash their hands with soap and water.
EVRYSDI® [risdiplam]
Distributed by:
Genentech USA, Inc.
A Member of the Roche Group
1 DNA Way
South San Francisco, CA 94080-4990
EVRYSDI is a registered trademark of Genentech, Inc.
©2026 Genentech, Inc. All rights reserved.
INSTRUCTIONS FOR USE
EVRYSDI® [ev-RIZ-dee]
(risdiplam)
for oral solution
Please read and understand this Instructions for Use and the Patient Information leaflet before you start taking EVRYSDI for information about EVRYSDI and how to prepare and give EVRYSDI through an oral syringe, gastrostomy tube (G-tube), or nasogastric tube (NG-tube).
If you have any questions about how to take EVRYSDI, contact your healthcare provider.
EVRYSDI should come as a liquid in a bottle when you receive it from the pharmacy. Do not take EVRYSDI and contact your pharmacist if the medicine in the bottle is a powder.
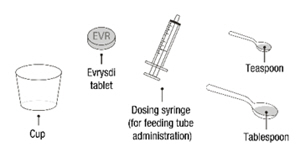
Each EVRYSDI carton contains (see Figure A):






Important information about EVRYSDI
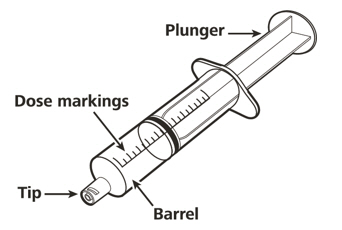
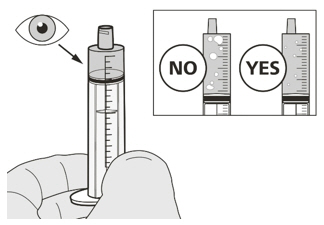
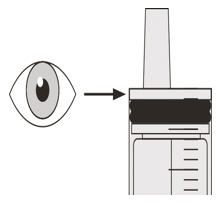
- Ask your healthcare provider to show you the correct oral syringe you should use and how to measure your prescribed daily dose.
- Always use the reusable oral syringes that come with EVRYSDI to measure your prescribed daily dose. If your carton does not contain two identical syringes, contact your pharmacist.
- Always take EVRYSDI exactly as your healthcare provider tells you to take it.
- Take EVRYSDI 1 time daily with or without a meal at approximately the same time each day.
- Do not take EVRYSDI if the bottle adapter is not in the bottle. If the bottle adapter is not in the bottle, contact your pharmacist.
- Do not mix EVRYSDI into food or liquids. Do not mix EVRYSDI with formula or milk.
- Do not take EVRYSDI if the bottle or oral syringes are damaged.
- Avoid getting EVRYSDI on your skin or in your eyes. If EVRYSDI gets on your skin, wash the area with soap and water. If EVRYSDI gets in your eyes, rinse your eyes with water.
- If you spill EVRYSDI, dry the area with a dry paper towel and then clean with water. Throw away the paper towel in the trash and wash your hands well with soap and water.
- If there is not enough EVRYSDI left in the bottle for your prescribed dose, throw away (discard) the bottle with remaining EVRYSDI and used oral syringes according to your local requirements.
- Use a new bottle of EVRYSDI to get your prescribed dose.
Do not mix EVRYSDI from the new bottle with the bottle you are currently using.
How to store EVRYSDI

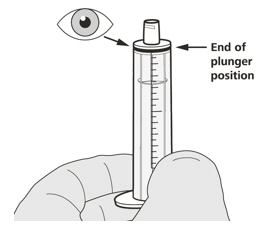
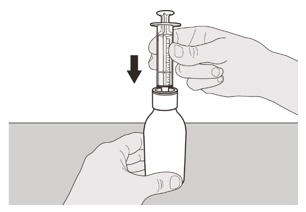
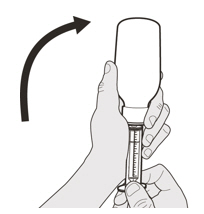
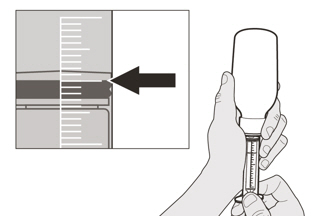
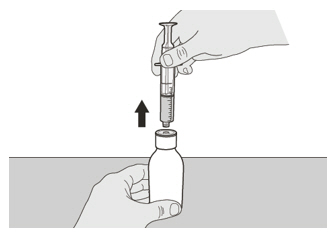
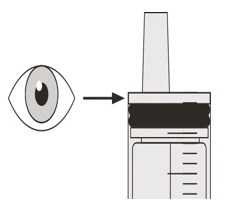
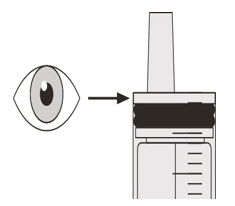
A) Preparing and withdrawing your dose
How to prepare your dose of EVRYSDI


If you are taking your dose of EVRYSDI by mouth, follow the instructions in " B) How to take a dose of EVRYSDI by mouth ".
If you are taking your dose of EVRYSDI through a gastrostomy tube, follow the instructions in " C) How to give a dose of EVRYSDI through a gastrostomy tube ".
If you are taking your dose of EVRYSDI through a nasogastric tube, follow the instructions in " D) How to give a dose of EVRYSDI through a nasogastric tube ".
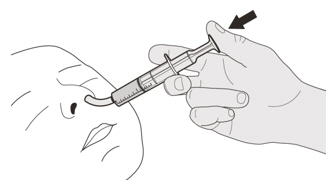
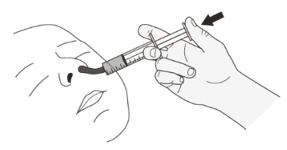
B) How to take a dose of EVRYSDI by mouth
Sit upright when taking a dose of EVRYSDI by mouth.


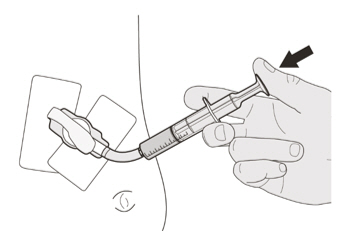
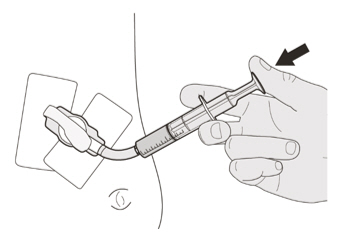
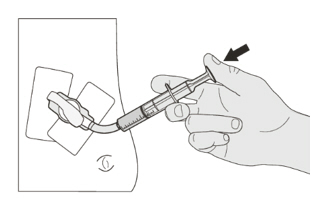
C) How to give a dose of EVRYSDI through a gastrostomy tube
If you are giving EVRYSDI through a gastrostomy tube, ask your healthcare provider to show you how to inspect the gastrostomy tube before giving EVRYSDI.
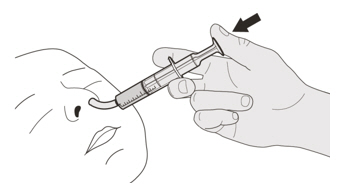
D) How to give a dose of EVRYSDI through a nasogastric tube
If you are giving EVRYSDI through a nasogastric tube, ask your healthcare provider to show you how to inspect the nasogastric tube before giving EVRYSDI.
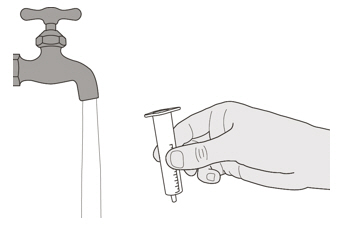
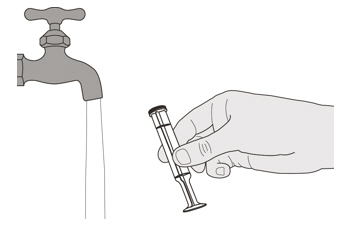
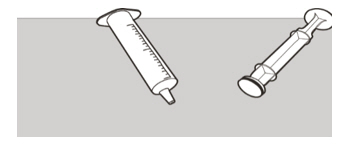
E) How to clean the oral syringe after use
EVRYSDI is a registered trademark of Genentech, Inc.
Distributed by:
Genentech, Inc.
1 DNA Way
South San Francisco, CA 94080-4990
Approved: 2/2025
This Instructions for Use has been Approved by the U.S. Food and Drug Administration.
©2025 Genentech, Inc. All Rights Reserved
EVRYSDI®
(risdiplam) for oral solution
Instructions for Constitution
(FOR HEALTHCARE PROVIDERS ONLY)
Each EVRYSDI carton contains (see Figure A):



Important information about EVRYSDI
- Do not use if the powder expiration date has passed. The powder expiration date is printed on the bottle label.
- Do not use the medicine if any of the supplies are damaged or missing.
- Use purified water to constitute the medicine.
- Select the appropriate oral syringes (1 mL, 6 mL, or 12 mL) based on the patient's dose and provide instruction to the patient/caregiver on how to administer their dose. The oral syringes provided in the carton are intended to be reusable.
- Only use the amber oral syringe provided for use with EVRYSDI. Other syringes may not be compatible with the press-in-bottle adapter and may not protect the product from light.
How to store EVRYSDI
- Store the dry powder at 20°C to 25°C (68°F to 77°F), excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP controlled room temperature]. Keep in the original carton.
- Store the constituted oral solution of EVRYSDI upright in the original amber bottle in a refrigerator at 2°C to 8°C (36°F to 46°F). Do not freeze.
Important precautions for preparation of EVRYSDI
- Avoid inhalation and direct contact with skin or mucous membranes with the dry powder and the constituted solution. If such contact occurs, wash thoroughly with soap and water; rinse eyes with water.
- Wear disposable gloves during the preparation and clean up procedure.
Constitution

Selecting the oral syringe for the prescribed daily dose of EVRYSDI
For the calculation of dosing volume, the syringe increments need to be considered. Round the dose volume to the closest increment marked on the selected oral syringe.
Select the correct oral syringe(s) (1 mL, 6 mL, or 12 mL) for the calculated dosing volume according to the table below and remove the other oral syringes.
Put the bottle back in its original carton with the correct oral syringes, Prescribing Information, and Instructions for Use.
Store the constituted oral solution of EVRYSDI upright in the original amber bottle in a refrigerator at 2°C to 8°C (36°F to 46°F). Do not freeze. Discard any unused portion 64 days after constitution.
EVRYSDI is a registered trademark of Genentech, Inc.
Distributed by:
Genentech, Inc.
1 DNA Way
South San Francisco, CA 94080-4990
Revision Date: 2/2025
©2025 Genentech, Inc. All Rights Reserved.
Representative sample of labeling (see the HOW SUPPLIED section for complete listing):
INSTRUCTIONS FOR USE
EVRYSDI® [ev-RIZ-dee]
(risdiplam)
Tablets, for oral use
Before you start
This Instructions for Use contains information on how to prepare and take EVRYSDI tablets.
Read this Instructions for Use and Patient Information leaflet before you start taking or giving EVRYSDI tablets for the first time and each time you get a refill. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or treatment.
If you have any questions about how to take EVRYSDI, contact your healthcare provider.
Important Information
- If you are taking EVRYSDI tablets, the daily dose is one tablet.
- EVRYSDI tablets can be swallowed whole with water. Do not chew, cut, or crush the tablet.
- If you are unable to swallow EVRYSDI tablets whole or have a nasogastric (NG) tube or gastrostomy tube (G-tube), your healthcare provider will show you how to prepare and take EVRYSDI tablets. Always take EVRYSDI tablets exactly as your healthcare provider tells you.
- Do not take or give EVRYSDI tablets until you have been shown the right way to prepare and take or give EVRYSDI.
- Wash your hands before and after preparing, taking or giving EVRYSDI.
- Check the expiration date and check the product for damage before use. Do not use if expired or damaged.
- Avoid getting the EVRYSDI tablet mixture on your skin or in your eyes. If the EVRYSDI tablet mixture gets on your skin, wash the area with soap and water. If the tablet mixture gets in your eyes, rinse your eyes with water.
- Keep the EVRYSDI tablet mixture out of sunlight.
- If you spill the EVRYSDI tablet mixture, dry the area with a dry paper towel and then clean with soap and water. Throw away the paper towel in the trash and wash your hands with soap and water.
- Do not take an extra dose if you vomit at any time after taking EVRYSDI.



Distributed by:
Genentech, USA Inc., A Member of the Roche Group
1 DNA Way, South San Francisco, CA 94080-4990
Evrysdi® is a registered trademark of Genentech, Inc.
©2026 Genentech, Inc.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Approved: 2/2026
PRINCIPAL DISPLAY PANEL - 60 mg/80 mL Bottle Carton
NDC 50242-175-07
Evrysdi®
(risdiplam)
for oral solution
60 mg/80 mL
(0.75 mg/mL)
Attention pharmacist: Evrysdi must be
constituted with water prior to dispensing.
80 mL (2.71 fl oz) total volume after constitution
Rx only
Genentech
11044976
PRINCIPAL DISPLAY PANEL - 5 mg Tablet Bottle Carton
NDC 50242-202-01
Evrysdi®
(risdiplam)
Tablets
5 mg
Do not chew, cut,
or crush tablet.
30 Tablets
Rx only
Genentech
11044980
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.