Design and created by Guideline Central in participation with the Consensus and Physician Experts and International Essential Tremor Foundation.

Essential Tremor in Adult Patients
Consensus and Physician Experts
International Essential Tremor Foundation
Publication Date: December 4, 2025
Overview/Background/Prevalence
- Essential Tremor (ET) is one of the most common movement disorders. It can occur at any age, but is most common in people age 40 and older where incidence increases with each decade. ET affects up to 5% of people over the age of 60.
- Age and family history are the two greatest risk factors for ET.
- ET is typically a slowly progressive condition with patients often having tremor for many years prior to seeking treatment.
- ET most commonly affects the hands but can affect the head and voice. Less commonly, the legs, trunk, jaw, and other facial muscles are involved.
- Patients report a beneficial effect of alcohol about 60% of the time.
- Many patients with ET have a family history of tremor (50%+). Despite this, while a few genes have been associated with ET, genetic testing is not currently available.
- ET is commonly misdiagnosed, and often confused with Parkinson’s disease (PD) or dystonia.
Assessment/Screening
- History should be taken to understand how tremor impacts daily living and function, to determine if treatment is indicated.
- Activities to ask about include eating, drinking, writing, hygiene, dressing, work, and hobbies.
- The social disability/stigma and embarrassment with ET can be significant, so this should be discussed.
- There are a number of scales that can be used to quantify the impact of tremor on the patient’s function. This includes: Bain and Findley Tremor ADL scale, TETRAS ADL scale and QUEST Essential Tremor Rating Scale. Some treatments may require these scales be performed to document medical necessity of the treatment.
- Neuroimaging to measure dopamine uptake (DaTscan) can be done if there is suspicion of underlying PD.
- Synuclein assays of tissue and fluids are now available, and emerging as a way to confirm underlying PD pathology.
- Examination of the patient includes assessment of the various parts of the body that can be affected.
Table 1. Examination for Essential Tremor
| Area | Comments |
|---|---|
| Limbs | Typically seen when holding a limb against gravity (arms outstretched, wing-beating) or with movement (finger to nose). These items together are called “action tremor,” reflecting the fact that ET typically occurs during movement and typically affects the upper extremities. |
| Head | Typically seen as a side to side shaking of the head (“no-no” tremor), but can occur in an up and down motion (“yes-yes”) or can be mixed. |
| Voice | The voice is evaluated by listening to speech but also by having the patient hold a prolonged “ahhh” or “eee.” |
| Facial Muscles | Examined by having the patient purse the lips or squeeze the eyelids. |
| Tasks | Patient can be observed during functional tasks such as writing, drawing, pouring water, drinking from a cup. |
- History should be taken to understand how tremor impacts daily living and function, to determine if treatment is indicated.
- Activities to ask about include eating, drinking, writing, hygiene, dressing, work, and hobbies.
- The social disability/stigma and embarrassment with ET can be significant, so this should be discussed.
- Neuroimaging to measure dopamine uptake (DaTscan) can be done if there is suspicion of underlying PD.
- Examination of the patient includes assessment of the various parts of the body that can be affected.
Differential Diagnosis
Parkinson's Disease
- Aspects of the tremor that suggest PD include unilateral tremor onset and notable rest tremor.
- Rest tremor often appears when the hand is down at the side, so walking should be part of a tremor evaluation.
- Rest tremor may also re-emerge after holding a posture for several seconds.
- Additionally, PD patients should demonstrate bradykinesia, and often rigidity of the limbs.
- Bradykinesia can be assessed by watching the patient do rapid repetitive movements such as finger tapping, hand opening/closing, and foot tapping.
- Patients with PD may have prodromal non-motor symptoms such as hyposmia and REM sleep behavior disorder, so these should be elicited.
Medications and Other Causes of Tremor
- The medication list should be reviewed carefully since medications such as stimulants, antidepressants, antipsychotics and many immunosuppressants can cause tremor.
- While most medications trigger tremor in a predictable dose-related fashion, there are some, like valproic acid and amiodarone, that can trigger tremor even after long-standing low-dosage exposure.
- When diagnosing ET, consider ruling out thyroid issues (e.g. hyperthyroidism) and metabolic disorders (e.g. B-12 deficiency).
- Also consider ruling out dystonic tremor, especially if tremor is present in or isolated to the head. Dystonia and ET are two movement disorders that may occur independently or coexist.
ET Plus
- For instance, many people with very long-standing ET may develop gait ataxia and rest tremor.
- Dystonic features (subtle posturing of the hands or head) can be seen in some people with ET.
- At this time, it is not known whether these are distinct neurological disorders different from classical ET but it seems likely that many, if not most, patients may evolve ET Plus features over time.
Table 2. Comparing Signs/Symptoms of ET and PD
| Essential Tremor | Parkinsonian Tremor |
|---|---|
| Most commonly affects upper limbs, head, voice | Most commonly affects upper limbs and less commonly lower limbs and jaw. Voice and head almost never affected |
| Typically bilateral | Begins unilateral and generally progresses to bilateral |
| Tremor primarily postural and kinetic (action tremor), rarely at rest | Tremor primarily at rest may have postural tremor (re-emergent), rarely kinetic |
| 4–12 Hz tremor | 3–6 Hz tremor |
| Tremor is primary symptom – slowness, stiffness, walking and balance problems are not commonly seen. | Slow movements (bradykinesia), rigidity (stiffness), and problems with walking or balance |
| Family history of tremor reported in the majority of patients | Rarely a family history (<20%) |
| Onset most common after 40 but can occur at any time in the lifespan | Average onset around 60 years, can be any time throughout adulthood |
| Alcohol often improves tremor | Alcohol does not improve tremor |
| Worsens with stress/emotion | Worsens with stress/emotion |
| About 8× more common than PD | Much less common than ET |
| DaTscan normal | DaTscan abnormal |
| Handwriting often large and tremulous | Handwriting often micrographic and not tremulous |
Management
Non-Pharmacological/Non-Surgical Treatment Options
Wrist-worn Non-invasive Stimulation
Transcutaneous Afferent Patterned Stimulation (TAPS)
- Cala kIQ is an individualized, calibrated, re-chargeable, non-invasive wrist-worn device to reduce tremor in a targeted arm. It provides electrical stimulation to the median and radial nerves through electrodes placed on the inside of a wrist band.
- The first generation TAPS system (Cala Trio) was cleared by the FDA in 2018. The most recent TAPS therapy system, Cala kIQ, was cleared in 2022. It is indicated in adults with essential tremor to provide transient relief of hand tremors following stimulation.
- The wrist band device is worn for 40 minutes, after which 64% of patients reported having persistent relief for an average of 94 minutes.
- When starting therapy, patients should choose an activity (e.g. eating) and use Cala kIQ 20–40 minutes prior. This usage should continue on-demand for at least 2 weeks to determine benefits.
- A typical charge will last for approximately 5 sessions. It takes approximately 3–4 hours to fully charge the device.
- It can be used with or without pharmacological therapies.
- Cala kIQ is contraindicated in patients with implanted electrical devices such as a pacemaker, defibrillator, or deep brain stimulation device; patients with a seizure disorder; pregnant women; and in persons with skin irritations, open wounds, or lesions on the wrist.
Transcutaneous Peripheral Nerve Stimulation (TPNS)
- Felix NeuroAI Wristband is a noninvasive, personalized, re-chargeable, transcutaneous neurostimulation system that provides artificial intelligence (AI) driven stimulation to the median, radial and ulnar nerves to continually optimize essential tremor in the upper limbs throughout the day.
- Felix NeuroAI Wristband was cleared by the FDA in 2025 for the treatment of essential tremor in adults and is indicated for alleviating tremor-related functional limitations in the upper limbs.
- Sensors continuously monitor tremor, sending data to a cloud-based AI algorithm that continually adjusts stimulation in real time based on an individual’s activity. In clinical studies, the device was worn for an average of 8.6 hours per day.
- Tremor improvement was reported in approximately 70-80% of patients by both clinicians and patients.
- A typical charge will last for one day of use. It takes approximately 5 hours to fully charge the device.
- It can be used with or without pharmacological therapies.
- In clinical trials, wearing a single device was shown to reduce tremors in both hands.
- Felix NeuroAI Wristband is contraindicated in patients with implanted electrical devices such as a pacemaker, defibrillator, or deep brain stimulation device; patients with a seizure disorder; pregnant women; and in persons with skin irritations, open wounds, or lesions on the wrist.
Pharmacological Treatment Options
- It has been estimated that 30–60% of persons with ET who tolerate current pharmacological treatment options have a reduction in tremor.
- Those that do respond to medications tend to have a 30–50% reduction in tremor.
- Tremor rarely completely resolves with medication.
- Limb tremor is generally the targeted tremor and tends to have a better and more consistent response than head or voice tremor.
Table 3. Currently Recommended Pharmacological Treatments for ET
| Drug | Class | Titration | Common Side Effects |
|---|---|---|---|
| Propranolol (the only FDA-approved medication for ET) (Level A) | Beta-blockera |
| Lightheadedness, bradycardia, fatigue, impotence, depression, nausea, weight gain, rash, diarrhea |
| Propranolol Long Acting (Level A) | Beta-blocker |
| Same as propranolol |
| Primidone (Level A) | Anticonvulsant |
| Sedation, fatigue, nausea, poor balance, dizziness, flu-like symptoms |
| Propranolol and primidone may be used in combination if tremor not well controlled with either alone | |||
| Gabapentin Monotherapy (Level B) Adjunct (insufficient evidence) | Anticonvulsant |
| Sedation, fatigue, dizziness, ataxia, nervousness, irritability, nausea, shortness of breath |
| Topiramate (Level B) | Anticonvulsant |
| Dizziness, disorientation, memory problems, loss of appetite, weight loss, paresthesia, fatigue, nausea, somnolence, headache |
| Alprazolam (Level B) Clonazepam (Level C) Diazepam Lorazepam | Benzodiazepines |
| Drowsiness, fatigue, lightheadedness, dizziness, depression, fatigue, loss of coordination, memory loss, confusion |
a Small studies have shown benefit from other beta-blockers such as atenolol (50–150 mg/day; Level B — probably effective), sotalol (75–200 mg/day; Level B — probably effective), and nadolol (120–240 mg/day; Level C — possibly effective), all of which could be tried in patients with ET
Acetazolamide, flunarizine, isoniazid, levetiracetam, pindolol, methazolamide, mirtazapine, nifedipine, trazodone, verapamil, and 3,4-diaminopyridine are not recommended for treatment of limb tremor in ET (AAN Guidelines).
There is insufficient evidence to make recommendations regarding the use of amantadine, clonidine, clozapine, gabapentin (adjunct therapy), glutethimide, L-tryptophan/pyridoxine, metoprolol, nicardipine, olanzapine, phenobarbital, pregabalin, quetiapine, theophylline and zonisamide in the treatment of limb tremor in ET (AAN Guidelines).
Surgical Treatment Options
Table 4. Surgical Treatment Options
| Deep Brain Stimulation (DBS) | Focused Ultrasound (FUS) | Gamma Knife Surgery (GKS) | |
|---|---|---|---|
| Surgical Method | Stimulation: an electrode is placed in the brain and connected to a pulse generator typically located in the chest to provide electrical stimulation to the brain. | Ablation: uses multiple ultrasound beams to destroy tissue in the brain. | Ablation: uses multiple radiation beams to destroy tissue in the brain |
| Brain Site | VIM nucleus of the thalamus | VIM nucleus of the thalamus | VIM nucleus of the thalamus |
| Status During Surgery | Awake or asleep under general anesthesia | Awake | Awake |
| Time to Benefit | Immediate | Immediate | Weeks to months |
| Pros |
|
|
|
| Cons |
|
|
|
| Outcomes |
| 35–75% tremor reduction (unilateral) 60–80% (staged bilateral) |
|
| Complications |
| Edema, headache, paresthesia, weakness, nausea, dysarthria, gait disturbances | Edema, scalp irritation, headache, fatigue, nausea, weakness, dysarthria, confusion |
Botulinum Toxins
- Botulinum toxin is not currently approved by the FDA for the treatment of tremor.
- General side effects of botulinum toxins include rash, pain, stiffness, cramping, hematoma, weakness, and paresthesia.
- Reports have shown efficacy of botulinum toxin for upper limb, head, and voice tremor when the tremor is not responding to oral pharmacotherapies.
Table 5. Botulinum Toxins in Various Tremors
| Area | Comments |
|---|---|
| Upper Limb | The greatest benefit has been shown to be between 6 and 16 weeks after the injections. Hand weakness is the most common side effect and is dose dependent. Focusing on the forearm wrist flexor instead of the extensor muscles significantly reduces weakness. |
| Head | It is important to distinguish ET from dystonic tremor. Botulinum toxins have been shown to be beneficial for both dystonic and ET head tremor in the majority of patients. The benefit usually occurs after one week and continues for 8–12 weeks. The most common side effects are dysphagia, headache and neck weakness. |
| Voice | 50–60% of patients have been reported to improve with botulinum toxin injections directed primarily at the vocal cord under electromyographic guidance or direct visualization with endoscopy. The most common side effects included weak voice, hoarseness, and breathy voice, all of which can last for several weeks. |
Assistive Devices
- According to the World Health Organization, assistive devices are tools which facilitate function.
- Assistive devices can enhance participation in meaningful activities and well-being.
- Assistive devices vary in complexity. These items can range from simple household items to those requiring advanced technology or software.
- When considering assistive devices, a formal evaluation is the initial step to identify individual needs and preferences and to determine the supports required and and barriers to use of an assistive device.
- A trial of the equipment is beneficial to determine effectiveness in meeting the individual’s goals.
- An occupational therapist is able to assist with concerns related to participation in daily activities, a physical therapist for concerns involving mobility or coordination, and a speech/language pathologist for concerns related to communication.
- Assistive devices (see Table 6 & 7) can be specific to the person, daily activity, or task.
- Many of these devices are also referred to as adaptive equipment or daily living aids. They help individuals complete everyday activities, thereby improving their quality of life.
Table 6. Assistive Devices
| Devices | Description | Attributes | Considerations |
|---|---|---|---|
| Exoskeletons | A wearable electromechanical device which detects rhythmic movements caused by the tremor and uses technology to produce a countermovement response | Reduces tremor power (40–80%) while the device is worn | Cost, bulkiness of the device, and discomfort when wearing are factors Level of evidence specific to efficacy of these devices remains low |
| Orthotics | Act in parallel with the affected body part to reduce tremor amplitude | Reduces tremor amplitude (up to 80%) when worn | Cost, availability, and bulkiness of the device are factors Level of evidence specific to efficacy of these devices remains low |
| Handheld Devices | Handheld devices with technology to counteract the motion of tremor | Reduces movement (71–76%) with Active Cancellation of Tremor technology | Cost associated with devices Works best for individuals with mild to moderate tremor |
| Limb Weights | Weights of an assessed optimal amount applied to either arms or legs to reduce tremor | Reduces tremor to improve function for some individuals | Level of evidence specific to efficacy of these devices remains low |
Table 7. Assistive Devices Specific to Daily Activities
| Devices | Examples | Attributes | Considerations |
|---|---|---|---|
| Dining Aids | Weighted utensils, rocker knife, covered spoon, plate guard, high sided dish, non-skid pad/surface, insulated weighted cup with lid, two handled cup, long reusable straw, stabilizing utensils |
|
|
| Grooming Aids | Hands-free hair dryer mount or stand, electric razor, electric toothbrush, long handled comb, suction cup toothbrush for dentures, tabletop nail clipper | ||
| Dressing Aids | Adapted clothing, magnetic button adaptors, weighted button aid and zipper pulls, elastic shoelaces | ||
| Bathing Aids | Wall mounted shampoo and soap dispensers, wash mitt, shower chair | ||
| Cooking Aids | Automatic jar opener, food processor, electric chopper, cut resistant gloves, adapted cutting board, pot stand | ||
| Writing Aids | Weighted pen or pencil, steadying aid for writing implement, adapted pen | ||
| Computer/Communication Aids | Mouse accessibility software, larger buttoned keyboard, keyguard, voice to text or text to speech software or phone application, fluency devices | ||
| Leisure Participation Aids | Card holder, large buttoned universal remote, book holder |
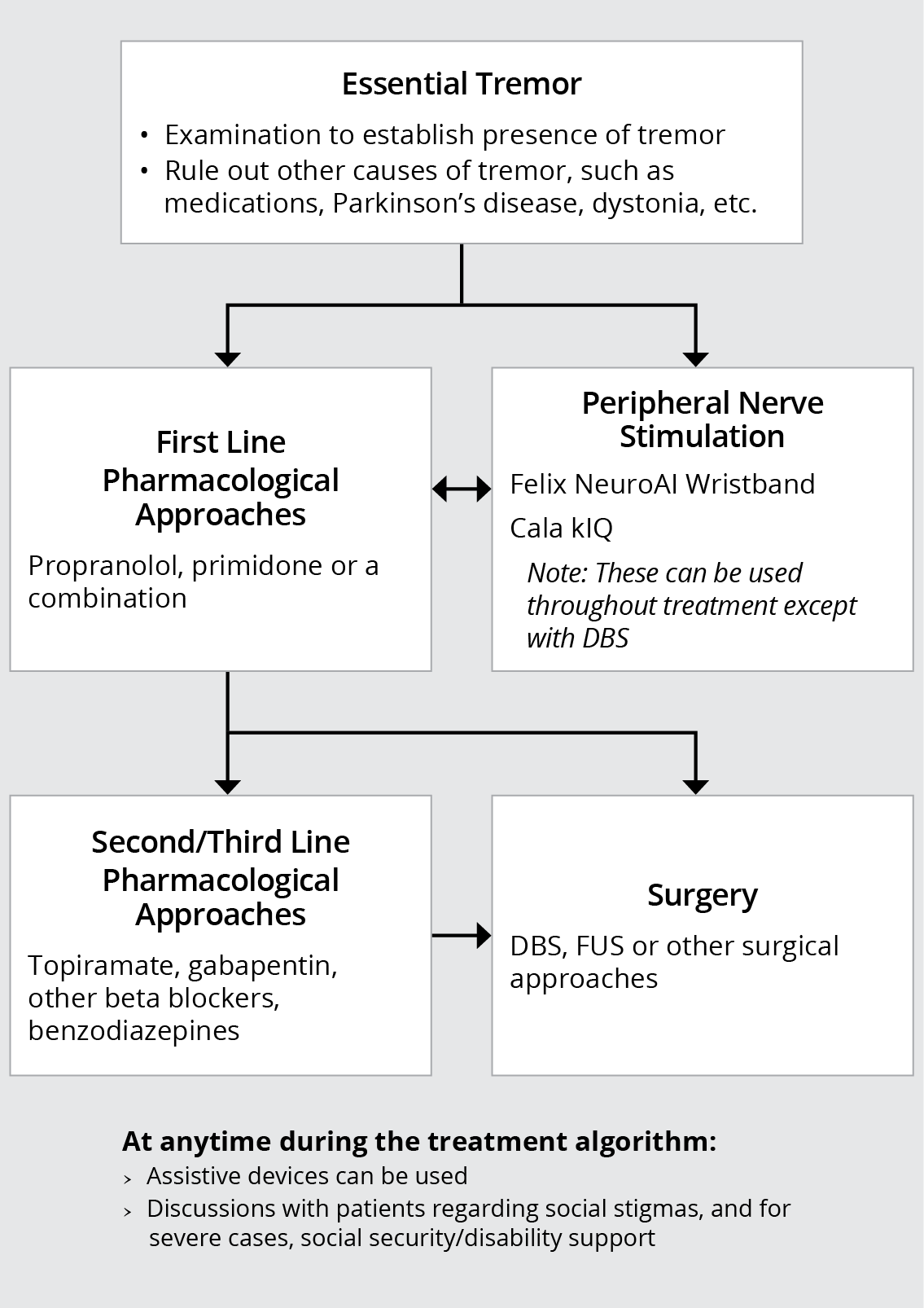
Figure 1. Overview of Management of Essential Tremor
Patient Tools/Resources
Patient/Clinician FAQ and Discussion Points
Q: What causes ET?
A: The cause of ET is currently unknown. A large percentage of persons with ET have a family history of the disorder.
Q: How is ET diagnosed?
A: There are no medical tests to confirm a diagnosis of ET. Generally, ET is diagnosed by ruling out other causes of tremor, including certain medications, Parkinson’s disease, and excessive stress or trauma.
Q: Is ET life-threatening?
A: While it can worsen over time, ET is not a life-threatening disorder. The severity of the tremor can vary from a barely noticeable tremor only present in situations of stress or anxiety, to a severe tremor that has a significant impact on activities of daily living.
Q: Can ET be “cured”?
A: There is currently no cure for ET; however there are a number of management approaches that can help improve quality of life.
Q: Which management approach is right for me?
A: Clinicians and patients should take a shared decision-making approach to identify which management strategies are right for each individual. Level of invasiveness, potential for side effects, efficacy, and cost can all be considered when deciding which approach(es) to start with.
Q: Will ET affect my ability to work?
A: It may. If your tremor is so severe that it disrupts your ability to work, you may qualify for federal disability benefits. The Social Security Administration administers two programs: Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI).
The International Essential Tremor Foundation (IETF) has a library of essential tremor materials available to healthcare providers and their patients. These include a comprehensive patient handbook, surgical options brochure and handouts focused on children with essential tremor, plus more. These resources are available at no charge. To learn more, visit EssentialTremor.org/physician-publication-order-form/
Abbreviations
- AAN
- Academy of Neurology
- DBS
- Deep brain stimulation
- ET
- essential tremor
- FUS
- focused ultrasound
- GKR
- gamma knife radiosurgery
- PD
- Parkinson's disease
- PET
- positron emission tomography
- SPECT
- single-photon emission computerized tomography
- TAPS
- transcutaneous afferent patterned stimulation
- TPNS
- transcutaneous peripheral nerve stimulation
- VIM
- ventral intermediate nucleus of thalamus
Expert Authors/Reviewers
Consultants:
Kelly E. Lyons,
Ph.D Holly Shill,
MD Rajesh Pahwa, MD
Disclaimer
This resource is for informational purposes only, intended as a quick-reference tool based on the cited source guideline(s), and should not be used as a substitute for the independent professional judgment of healthcare providers. Practice guidelines are unable to account for every individual variation among patients or take the place of clinician judgment, and the ultimate decision concerning the propriety of any course of conduct must be made by healthcare providers after consideration of each individual patient situation. Guideline Central does not endorse any specific guideline(s) or guideline recommendations and has not independently verified the accuracy hereof. Any use of this resource or any other Guideline Central resources is strictly voluntary.
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.