Key Points
- Disease stages in patients with valvular heart disease should be classified (Stages A, B, C, and D) on the basis of symptoms, valve anatomy, the severity of valve dysfunction, and the response of the ventricle and pulmonary circulation.
- In the evaluation of a patient with valvular heart disease, history and physical examination findings should be correlated with the results of noninvasive testing (i.e., ECG, chest x-ray, transthoracic echocardiogram). If there is discordance between the physical examination and initial noninvasive testing, consider further noninvasive (computed tomography, cardiac magnetic resonance imaging, stress testing) or invasive (transesophageal echocardiography, cardiac catheterization) testing to determine optimal treatment strategy.
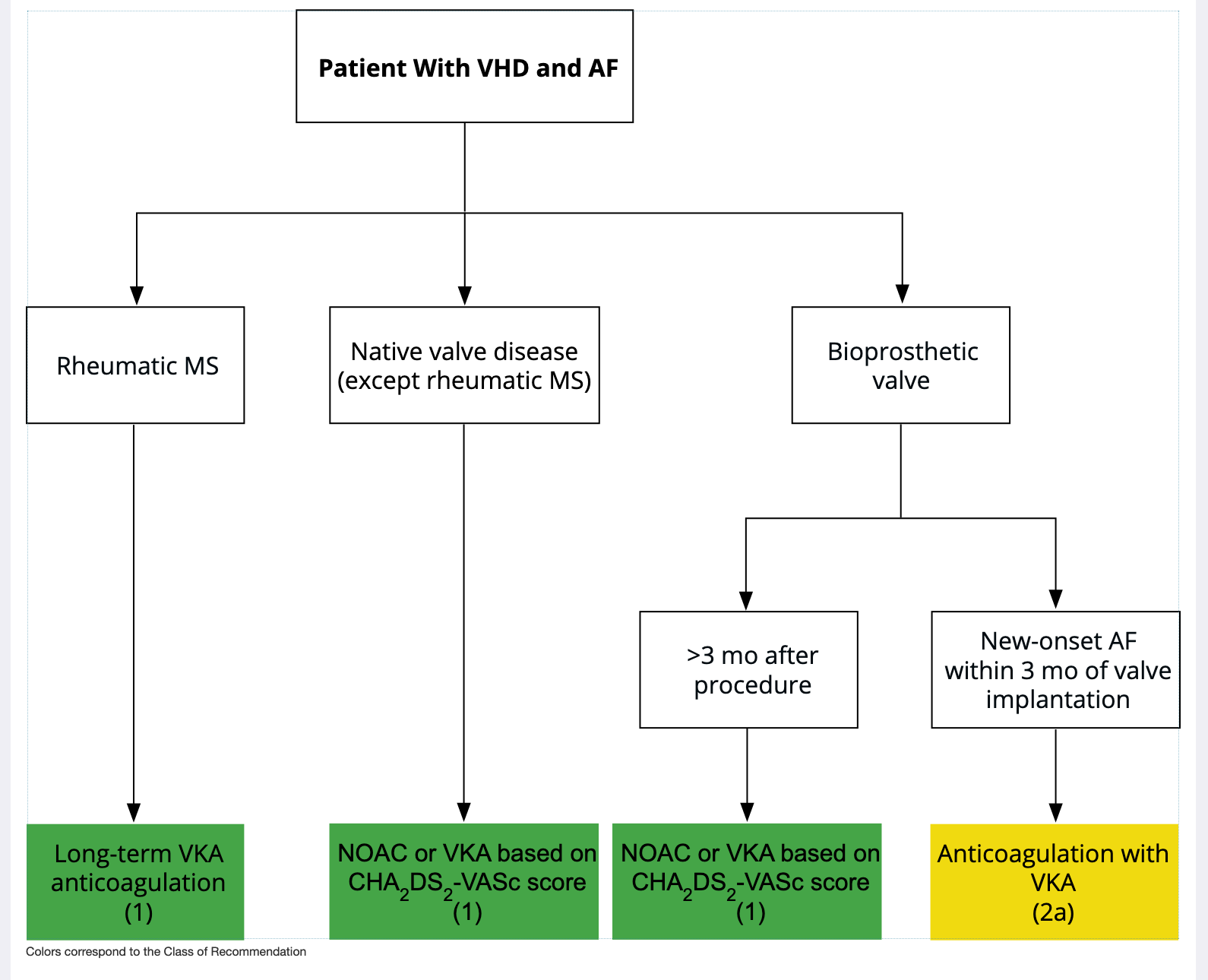
- For patients with valvular heart disease and atrial fibrillation (except for patients with rheumatic mitral stenosis or a mechanical prosthesis), the decision to use oral anticoagulation to prevent thromboembolic events, with either a vitamin K antagonist or a non–vitamin K antagonist anticoagulant, should be made in a shared decision-making process based on the CHA2DS2-VASc score. Patients with rheumatic mitral stenosis or a mechanical prosthesis and atrial fibrillation should receive oral anticoagulation with a vitamin K antagonist.
- All patients with severe valvular heart disease being considered for valve intervention should be evaluated by a multidisciplinary team, with either referral to or consultation with a Primary or Comprehensive Valve Center.
- Treatment of severe aortic stenosis with either a transcatheter or surgical valve prosthesis should be based primarily on symptoms or reduced ventricular systolic function. Earlier intervention may be considered if indicated by results of exercise testing, biomarkers, rapid progression, or the presence of very severe stenosis.
- Indications for transcatheter aortic valve implantation are expanding AS a result of multiple randomized trials of transcatheter aortic valve implantation atrioversus surgical aortic valve replacement. The choice of type of intervention for a patient with severe aortic stenosis should be a shared decision-making process that considers the lifetime risks and benefits associated with type of valve (mechanical versus bioprosthetic) and type of approach (transcatheter versus surgical).
- Indications for intervention for valvular regurgitation are relief of symptoms and prevention of the irreversible long-term consequences of left ventricular volume overload. Thresholds for intervention now are lower than they were previously because of more durable treatment options and lower procedural risks.
- A mitral transcatheter edge-to-edge repair is of benefit to patients with severely symptomatic primary mitral regurgitation who are at high or prohibitive risk for surgery, AS well AS to a select subset of patients with secondary mitral regurgitation who remain severely symptomatic despite guideline-directed management and therapy for heart failure.
- Patients presenting with severe symptomatic isolated tricuspid regurgitation, commonly associated with device leads and atrial fibrillation, may benefit from surgical intervention to reduce symptoms and recurrent hospitalizations if done before the onset of severe right ventricular dysfunction or end-organ damage to the liver and kidney.
- Bioprosthetic valve dysfunction may occur because of either degeneration of the valve leaflets or valve thrombosis. Catheter-based treatment for prosthetic valve dysfunction is reasonable in selected patients for bioprosthetic leaflet degeneration or paravalvular leak in the absence of active infection.
Treatment
Table 1. Evaluation of Patients With Known or Suspected VHD
* TTE is the standard initial diagnostic test in the initial evaluation of patients with known or suspected VHD.
Table 2. Stages of Progression of VHD
Table 3. Frequency of Echocardiograms in Asymptomatic Patients With VHD and Normal Left Ventricular (LV) Function
Patients with mixed valve disease may require serial evaluations at intervals earlier than recommended for single-valve lesions. These intervals apply to most patients with each valve lesion and do not take into consideration the etiology of the valve disease.
* With normal stroke volume.
Table 4. Secondary Prevention of Rheumatic Fever
* In patients with documented valvular heart disease, the duration of rheumatic fever prophylaxis should be ≥10 y or until the patient is 40 y of age (whichever is longer). Lifelong prophylaxis may be recommended if the patient is at high risk of group A streptococcus exposure. Secondary rheumatic heart disease prophylaxis is required even after valve replacement.
† Administration every 3 wk is recommended in certain high-risk situations.
‡ Macrolide antibiotics should not be used in persons taking other medications that inhibit cytochrome P450 3A, such as azole antifungal agents, HIV protease inhibitors, and some selective serotonin reuptake inhibitors. Table 5. Duration of Secondary Prophylaxis for Rheumatic Fever
* Lifelong prophylaxis may be recommended if the patient is at high risk of group A streptococcus exposure. Secondary rheumatic heart disease prophylaxis is required even after valve replacement.
† Clinical or echocardiographic evidence.
2.4.1. Secondary Prevention of Rheumatic Fever
In patients with rheumatic heart disease, secondary prevention of rheumatic fever is indicated (Tables 4 and 5). ( C-EO, I )
2.4.2. IE Prophylaxis
Antibiotic prophylaxis is reasonable before dental procedures that involve manipulation of gingival tissue, manipulation of the periapical region of teeth, or perforation of the oral mucosa in patients with
VHD who have any of the following:
- Prosthetic cardiac valves, including transcatheter-implanted prostheses and homografts.
- Prosthetic material used for cardiac valve repair, such AS annuloplasty rings, chords, or clips.
- Previous IE.
- Unrepaired cyanotic congenital heart disease or repaired congenital heart disease, with residual shunts or valvular regurgitation at the site of or adjacent to the site of a prosthetic patch or prosthetic device.
- Cardiac transplant with valve regurgitation attributable to a structurally abnormal valve.
( C-LD, IIa ) In patients with VHD who are at high risk of IE, antibiotic prophylaxis is not recommended for nondental procedures (e.g., TEE, esophagogastroduodenoscopy, colonoscopy, or cystoscopy) in the absence of active infection. ( B-NR, III (no benefit) )
2.4.3. Anticoagulation for AF in Patients With VHD
For patients with
AF and native valve heart disease (except rheumatic mitral stenosis [
MS]) or who received a bioprosthetic valve >3 months ago, a non-
vitamin K oral anticoagulant (
NOAC) is an effective alternative to
VKA anticoagulation and should be administered on the basis of the patient’s CHA2DS2 VASc score.
( A, I ) For patients with
AF and rheumatic
MS, long-term
VKA oral anticoagulation is recommended.
( C-EO, I ) For patients with new-onset
AF ≤3 months after surgical or transcatheter bioprosthetic valve replacement, anticoagulation with a
VKA is reasonable.
( B-NR, IIa ) In patients with mechanical heart valves with or without
AF who require long-term anticoagulation with
VKA to prevent valve thrombosis, NOACs are not recommended.
( B-R, III (harm) ) Figure 1. Anticoagulation for AF in Patients With VHD
2.5. Evaluation of Surgical and Interventional Risk
For patients with VHD for whom intervention is contemplated, individual risks should be calculated for specific surgical and/or transcatheter procedures, using online tools when available, and discussed before the procedure AS a part of a shared decision-making process. ( C-EO, I )
Table 6. Risk Assessment for Surgical Valve Procedures
* Use of the STS Predicted Risk of Mortality (http://riskcalc.sts.org/stswebriskcalc/#/) to predict risk in a given institution with reasonable reliability is appropriate only if institutional outcomes are within 1 standard deviation of the STS average observed/expected mortality ratio for the procedure in question. The EUROSCORE II risk calculator may also be considered for use and is available at http://www.euroscore.org/calc.html.
† Seven frailty indices: Katz Activities of Daily Living (independence in feeding, bathing, dressing, transferring, toileting, and urinary continence) plus independence in ambulation (no walking aid or assistance required, or completion of a 5-m walk in <6 s). Other scoring systems can be applied to calculate no, mild, or moderate to severe frailty.
Examples of major organ system compromise include cardiac dysfunction (severe LV systolic or diastolic dysfunction or RV dysfunction, fixed pulmonary hypertension); kidney dysfunction (chronic kidney disease, stage 3 or worse); pulmonary dysfunction (FEV1 <50% or D <50% of predicted); central nervous system dysfunction (dementia, Alzheimer’s disease, Parkinson’s disease, cerebrovascular accident with persistent physical limitation); gastrointestinal dysfunction (Crohn’s disease, ulcerative colitis, nutritional impairment, or serum albumin <3.0); cancer (active malignancy); and liver dysfunction (any history of cirrhosis, variceal bleeding, or elevated INR in the absence of VKA therapy).
§ Examples of procedure-specific impediments include presence of tracheostomy, heavily calcified (porcelain) ascending aorta, chest malformation, arterial coronary graft adherent to posterior chest wall, and radiation damage. Table 7. Examples of Procedure-Specific Risk Factors for Interventions Not Incorporated Into Existing Risk Scores
* Validated frailty scores include the Katz Activities of Daily Living Score
Table 8. Median Operative Mortality Rates for Specific Surgical Procedures (STS Adult Cardiac Surgery Database, 2019
2.6. The Multidisciplinary Heart Valve Team and Heart Valve Centers
Patients with severe VHD should be evaluated by a Multidisciplinary Heart Valve Team (MDT) when intervention is considered. ( C-EO, I )
Consultation with or referral to a Primary or Comprehensive Heart Valve Center is reasonable when treatment options are being discussed for 1) asymptomatic patients with severe VHD, 2) patients who may benefit from valve repair versus valve replacement, or 3) patients with multiple comorbidities for whom valve intervention is considered. ( C-LD, IIa )
Table 9. Structure of Primary and Comprehensive Valve Centers
* A Primary (Level II) Center may provide additional procedures traditionally offered at a Comprehensive (Level I) Center as long as the criteria for competence and outcomes are met.
† If intraoperative imaging and surgical expertise exist.
‡ If mitral valve anatomy is not suitable for valve repair.
§ Equipped with a fixed radiographic imaging system and flat-panel fluoroscopy, offering catheterization laboratory-quality imaging and hemodynamic capability. Used with permission from Nishimura et al. J Am Coll Cardiol. 2019;73:2609-35.
2.7.4. Periodic Imaging After Valve Intervention
In asymptomatic patients with any type of valve intervention, a baseline postprocedural TTE followed by periodic monitoring with TTE is recommended, depending on type of intervention, length of time after intervention, ventricular function, and concurrent cardiac conditions. ( C-EO, I )
Table 10. Timing of Periodic Imaging After Valve Intervention
Imaging Follow-Up*
* Initial postprocedural TTE is recommended for all patients, ideally 1 to 3 months after the procedure. Annual clinical follow-up is recommended annually for all patients after valve intervention at a Primary or Comprehensive Valve Center.
† Repeat imaging is appropriate at shorter follow-up intervals for changing signs or symptoms, during pregnancy, and to monitor residual or concurrent cardiac dysfunction.
‡ Imaging may be done more frequently in patients with bioprosthetic surgical valves if there are risk factors for early valve degeneration (e.g., younger age, renal failure, diabetes)* Initial postprocedural TTE is recommended for all patients, ideally 1 to 3 months after the procedure. Annual clinical follow-up is recommended annually for all patients after valve intervention at a Primary or Comprehensive Valve Center.
† Repeat imaging is appropriate at shorter follow-up intervals for changing signs or symptoms, during pregnancy, and to monitor residual or concurrent cardiac dysfunction.
‡ Imaging may be done more frequently in patients with bioprosthetic surgical valves if there are risk factors for early valve degeneration (e.g., younger age, renal failure, diabetes)
3.2.1.1. Diagnostic Testing: Initial Diagnosis
In patients with signs or symptoms of AS or a BAV, TTE is indicated for accurate diagnosis of the cause of AS, assessment of hemodynamic severity, measurement of LV size and systolic function, and determination of prognosis and timing of valve intervention. ( A, I )
In patients with suspected low-flow, low-gradient severe AS with normal LVEF (Stage D3), optimization of blood pressure control is recommended before measurement of AS severity by TTE, TEE, cardiac catheterization, or CMR. ( B-NR, I )
In patients with suspected low-flow, low-gradient severe AS with reduced LVEF (Stage D2), low-dose dobutamine stress testing with echocardiographic or invasive hemodynamic measurements is reasonable to further define severity and assess contractile reserve. ( B-NR, IIa )
In patients with suspected low-flow, low-gradient severe AS with normal or reduced LVEF (Stages D2 and D3), calculation of the ratio of the outflow tract to aortic velocity is reasonable to further define severity. ( B-NR, IIa )
In patients with suspected low-flow, low-gradient severe AS with normal or reduced LVEF (Stages D2 and D3), measurement of aortic valve calcium score by CT imaging is reasonable to further define severity. ( B-NR, IIa )
3.2.1.5. Diagnostic Testing: Exercise Testing
In asymptomatic patients with severe AS (Stage C1), exercise testing is reasonable to assess physiological changes with exercise and to confirm the absence of symptoms. ( B-NR, IIa )
In symptomatic patients with severe AS (Stage D1, aortic velocity ≥4.0 m/s or mean pressure gradient ≥40 mm Hg), exercise testing should not be performed because of the risk of severe hemodynamic compromise ( B-NR, III (harm) )
3.2.2. Medical Therapy
In patients at risk of developing AS (Stage A) and in patients with asymptomatic AS (Stages B and C), hypertension should be treated according to standard GDMT, started at a low dose, and gradually titrated upward as needed, with appropriate clinical monitoring. ( B-NR, I )
In all patients with calcific AS, statin therapy is indicated for primary and secondary prevention of atherosclerosis on the basis of standard risk scores. ( A, I )
In patients who have undergone
TAVI, renin–angiotensin system blocker therapy (
ACE inhibitor or
ARB) may be considered to reduce the long-term risk of all-cause mortality.
( B-NR, IIb ) In patients with calcific AS (Stages B and C), statin therapy is not indicated for prevention of hemodynamic progression of AS. ( A, III (no benefit) )
3.2.3. Timing of Intervention
In adults with severe high-gradient AS (Stage D1) and symptoms of exertional dyspnea, HF, angina, syncope, or presyncope by history or on exercise testing, AVR is indicated. ( A, I )
In asymptomatic patients with severe AS and an LVEF <50% (Stage C2), AVR is indicated. ( B-NR, I )
In asymptomatic patients with severe AS (Stage C1) who are undergoing cardiac surgery for other indications, AVR is indicated. ( B-NR, I )
In symptomatic patients with low-flow, low-gradient severe AS with reduced LVEF (Stage D2), AVR is recommended. ( B-NR, I )
In symptomatic patients with low-flow, low-gradient severe AS with normal LVEF (Stage D3), AVR is recommended if AS is the most likely cause of symptoms. ( B-NR, I )
In apparently asymptomatic patients with severe AS (Stage C1) and low surgical risk, AVR is reasonable when an exercise test demonstrates decreased exercise tolerance (normalized for age and sex) or a fall in systolic blood pressure of ≥10 mm Hg from baseline to peak exercise. ( B-NR, IIa )
In asymptomatic patients with very severe AS (defined AS an aortic velocity of ≥5 m/s) and low surgical risk, AVR is reasonable. ( B-R, IIa )
In apparently asymptomatic patients with severe AS (Stage C1) and low surgical risk, AVR is reasonable when the serum B-type natriuretic peptide (BNP) level is >3 times normal. ( B-NR, IIa )
In asymptomatic patients with high-gradient severe AS (Stage C1) and low surgical risk, AVR is reasonable when serial testing shows an increase in aortic velocity ≥0.3 m/s per year. ( B-NR, IIa )
In asymptomatic patients with severe high-gradient AS (Stage C1) and a progressive decrease in LVEF on at least 3 serial imaging studies to <60%, AVR may be considered. ( B-NR, IIb )
In patients with moderate AS (Stage B) who are undergoing cardiac surgery for other indications, AVR may be considered. ( C-EO, IIb )
Figure 2. Timing of Intervention for AS

Colors correspond to the Class of Recommendation.
Arrows show the decision pathways that result in a recommendation for AVR. Periodic monitoring is indicated for all patients in whom AVR is not yet indicated, including those with asymptomatic (Stage C) and symptomatic (Stage D) AS and those with low-gradient AS (Stage D2 or D3) who do not meet the criteria for intervention.
See Section 3.2.4 for choice of valve type (mechanical versus bioprosthetic [TAVR or SAVR]) when AVR is indicated.
3.2.4.1. Choice of Mechanical Versus Bioprosthetic AVR
In patients with an indication for AVR, the choice of prosthetic valve should be based on a shared decision-making process that accounts for the patient’s values and preferences and includes discussion of the indications for and risks of anticoagulant therapy and the potential need for and risks associated with valve reintervention. ( C-EO, I )
For patients of any age requiring
AVR for whom
VKA anticoagulant therapy is contraindicated, cannot be managed appropriately, or is not desired, a bioprosthetic
AVR is recommended.
( C-EO, I ) For patients <50 years of age who do not have a contraindication to anticoagulation and require AVR, it is reasonable to choose a mechanical aortic prosthesis over a bioprosthetic valve. ( B-R, IIa )
For patients 50 to 65 years of age who require AVR and who do not have a contraindication to anticoagulation, it is reasonable to individualize the choice of either a mechanical or bioprosthetic AVR with consideration of individual patient factors and after informed shared decision-making. ( B-NR, IIa )
In patients >65 years of age who require AVR, it is reasonable to choose a bioprosthesis over a mechanical valve. ( B-R, IIa )
In patients <50 years of age who prefer a bioprosthetic AVR and have appropriate anatomy, replacement of the aortic valve by a pulmonic autograft (the Ross procedure) may be considered at a Comprehensive Valve Center. ( B-NR, IIb )
3.2.4.2. Choice of SAVR Versus TAVI for Patients for Whom a Bioprosthetic AVR Is Appropriate
For symptomatic and asymptomatic patients with severe AS and any indication for AVR who are <65 years of age or have a life expectancy >20 years, SAVR is recommended. ( A, I )
For symptomatic patients with severe AS who are 65 to 80 years of age and have no anatomic contraindication to transfemoral TAVI, either SAVR or transfemoral TAVI is recommended after shared decision-making about the balance between expected patient longevity and valve durability. ( A, I )
For symptomatic patients with severe AS who are >80 years of age or for younger patients with a life expectancy <10 years and no anatomic contraindication to transfemoral TAVI, transfemoral TAVI is recommended in preference to SAVR. ( A, I )
In asymptomatic patients with severe AS and an LVEF <50% who are ≤80 years of age and have no anatomic contraindication to transfemoral TAVI, the decision between TAVI and SAVR should follow the same recommendations AS for symptomatic patients in Recommendations 1, 2, and 3 above. ( B-NR, I )
For asymptomatic patients with severe AS and an abnormal exercise test, very severe AS, rapid progression, or an elevated BNP (COR 2a indications for AVR), SAVR is recommended in preference to TAVI. ( B-NR, I )
For patients with an indication for AVR for whom a bioprosthetic valve is preferred but valve or vascular anatomy or other factors are not suitable for transfemoral TAVI, SAVR is recommended. ( A, I )
For symptomatic patients of any age with severe AS and a high or prohibitive surgical risk, TAVI is recommended if predicted post-TAVI survival is >12 months with an acceptable quality of life. ( A, I )
For symptomatic patients with severe AS for whom predicted post-TAVI or post-SAVR survival is <12 months or for whom minimal improvement in quality of life is expected, palliative care is recommended after shared decision-making, including discussion of patient preferences and values. ( C-EO, IIb )
In critically ill patients with severe AS, percutaneous aortic balloon dilation may be considered AS a bridge to SAVR or TAVI. ( C-EO, IIb )
Figure 3. Choice of SAVR Versus TAVI When AVR is Indicated for Valvular AS

Colors correspond to the Class of Recommendation.
* Approximate ages, based on US Actuarial Life Expectancy tables, are provided for guidance. The balance between expected patient longevity and valve durability varies continuously across the age range, with more durable valves preferred for patients with a longer life expectancy. Bioprosthetic valve durability is finite (with shorter durability for younger patients) whereas mechanical valves are very durable but require life-long anticoagulation. Long-term (20 year) data on outcomes with surgical bioprosthetic valves is available; robust data on transcatheter bioprosthetic valves only extends to 5 years leading to uncertainty about longer term outcomes. The decision about valve type should be individualized based on patient specific factors that might affect expected longevity.
† Placement of a transcatheter valve requires vascular anatomy that allows transfemoral delivery and the absence of aortic root dilation that would require surgical replacement. Valvular anatomy must be suitable for placement of the specific prosthetic valve including annulus size and shape, leaflet number and calcification and coronary ostial height. See ACC Expert Consensus Statement.
Table 12. A Simplified Framework With Examples of Factors Favoring SAVR, TAVI, or Palliation Instead of Aortic Valve Intervention
* Expected remaining years of life can be estimated from U.S. Actuarial Life Expectancy tables. The balance between expected patient longevity and valve durability varies continuously across the age range, with more durable valves preferred for patients with a longer life expectancy. Bioprosthetic valve durability is finite (with shorter durability for younger patients), whereas mechanical valves are very durable but require lifelong anticoagulation. Long-term (20-y) data on outcomes with surgical bioprosthetic valves are available; robust data on transcatheter bioprosthetic valves extend only to 5 y, leading to uncertainty about longer-term outcomes. The decision about valve type should be individualized on the basis of patient-specific factors that might affect expected longevity.
† A large aortic annulus may not be suitable for currently available transcatheter valve sizes. With a small aortic annulus or aorta, a surgical annulus-enlarging procedure may be needed to allow placement of a larger prosthesis and avoid patient–prosthesis mismatch.
‡ Dilation of the aortic sinuses or ascending aorta may require concurrent surgical replacement, particularly in younger patients with a BAV.
Aortic Regurgitation
Table 13. Stages of Chronic Aortic Regurgitation (AR)
4.3.1. Diagnosis of Chronic AR
In patients with signs or symptoms of AR, TTE is indicated for assessment of the cause and severity of regurgitation, LV size and systolic function, prognosis, and timing of valve intervention. ( B-NR, I )
In patients with a BAV or with known dilation of the aortic sinuses or ascending aorta, TTE is indicated to evaluate the presence and severity of AR. ( B-NR, I )
In patients with moderate or severe AR and suboptimal TTE images or a discrepancy between clinical and TTE findings, TEE, CMR, or cardiac catheterization is indicated for the assessment of LV systolic function, systolic and diastolic volumes, aortic size, and AR severity. ( B-NR, I )
4.3.2. Medical Therapy
In asymptomatic patients with chronic AR (Stages B and C), treatment of hypertension (systolic blood pressure >140 mm Hg) is recommended. ( B-NR, I )
In patients with severe
AR who have symptoms and/or
LV systolic dysfunction (Stages C2 and D) but a prohibitive surgical risk,
GDMT for reduced
LVEF with
ACE inhibitors, ARBs, and/or
sacubitril/valsartan is recommended.
( B-NR, I )
4.3.3. Timing of Intervention
In symptomatic patients with severe AR (Stage D), aortic valve surgery is indicated regardless of LV systolic function. ( B-NR, I )
In asymptomatic patients with chronic severe AR and LV systolic dysfunction (LVEF ≤55%) (Stage C2), aortic valve surgery is indicated if no other cause for systolic dysfunction is identified. ( B-NR, I )
In patients with severe AR (Stage C or D) who are undergoing cardiac surgery for other indications, aortic valve surgery is indicated. ( C-EO, I )
In asymptomatic patients with severe AR and normal LV systolic function (LVEF >55%), aortic valve surgery is reasonable when the LV is severely enlarged (LVESD >50 mm or indexed LVESD 25 mm/m) (Stage C2). ( B-NR, IIa )
In patients with moderate AR (Stage B) who are undergoing cardiac or aortic surgery for other indications, aortic valve surgery is reasonable. ( C-EO, IIa )
In asymptomatic patients with severe AR and normal LV systolic function at rest (LVEF >55%; Stage C1) and low surgical risk, aortic valve surgery may be considered when there is a progressive decline in LVEF on at least 3 serial studies to the low–normal range (LVEF 55% to 60%) or a progressive increase in LV dilation into the severe range (LV end-diastolic dimension [LVEDD] 65 mm). ( B-NR, IIb )
In patients with isolated severe AR who have indications for SAVR and are candidates for surgery, TAVI should not be performed. ( B-NR, III (harm) )
Figure 4. Timing of Intervention for AR

Colors correspond to the Class of Recommendation.
Bicuspid Aortic Valve
5.1.1.1. Diagnostic Testing: Initial Diagnosis
In patients with a known BAV, TTE is indicated to evaluate valve morphology, measure severity of AS and AR, assess the shape and diameter of the aortic sinuses and ascending aorta, and evaluate for the presence of aortic coarctation for prediction of clinical outcome and to determine timing of intervention. ( B-NR, I )
In patients with BAV, CMR angiography or CT angiography is indicated when morphology of the aortic sinuses, sinotubular junction, or ascending aorta cannot be assessed accurately or fully by echocardiography. ( C-LD, I )
In first-degree relatives of patients with a known BAV, a screening TTE might be considered to look for the presence of a BAV or asymptomatic dilation of the aortic sinuses and ascending aorta. ( B-NR, IIb )
Figure 5. Intervals for Imaging the Aorta in Patients With a BAV

Colors correspond to the Class of Recommendation.
5.1.1.2. Diagnostic Testing: Routine Follow-Up
In patients with BAV and a diameter of the aortic sinuses or ascending aorta of ≥4.0 cm, lifelong serial evaluation of the size and morphology of the aortic sinuses and ascending aorta by echocardiography, CMR, or CT angiography is reasonable, with the examination interval determined by the degree and rate of progression of aortic dilation and by family history. ( C-LD, IIa )
In patients with a BAV who have undergone AVR, continued lifelong serial interval imaging of the aorta is reasonable if the diameter of the aortic sinuses or ascending aorta is ≥4.0 cm. ( B-NR, IIa )
5.1.2.1. Intervention: Replacement of the Aorta in Patients with BAV
In asymptomatic or symptomatic patients with a BAV and a diameter of the aortic sinuses or ascending aorta >5.5 cm, operative intervention to replace the aortic sinuses and/or the ascending aorta is recommended. ( B-NR, I )
In asymptomatic patients with a BAV, a diameter of the aortic sinuses or ascending aorta of 5.0 to 5.5 cm, and an additional risk factor for dissection (e.g., family history of aortic dissection, aortic growth rate >0.5 cm per year, aortic coarctation), operative intervention to replace the aortic sinuses and/or the ascending aorta is reasonable if the surgery is performed at a Comprehensive Valve Center. ( B-NR, IIa )
In patients with a BAV with indications for SAVR and a diameter of the aortic sinuses or ascending aorta ≥4.5 cm, replacement of the aortic sinuses and/or ascending aorta is reasonable if the surgery is performed at a Comprehensive Valve Center. ( B-NR, IIa )
In patients with a BAV who meet criteria for replacement of the aortic sinuses, valve-sparing surgery may be considered if the surgery is performed at a Comprehensive Valve Center. ( C-LD, IIb )
In asymptomatic patients with a BAV who are at low surgical risk, have a diameter of the aortic sinuses or ascending aorta of 5.0 to 5.5 cm, and have no additional risk factors for dissection, operative intervention to replace the aortic sinuses and/or the ascending aorta may be considered if the surgery is performed at a Comprehensive Valve Center. ( B-NR, IIb )
Figure 6. Intervention for Replacement of the Aorta in Patients With a BAV

* Family history of aortic dissection, aortic growth rate ≥0.5 cm per year, presence of aortic coarctation.
Colors correspond to the Class of Recommendation.
5.1.2.2. Intervention: Replacement of the Aortic Valve
In patients with BAV and severe AR who meet criteria for AVR, aortic valve repair may be considered in selected patients if the surgery is performed at a Comprehensive Valve Center. ( C-LD, IIb )
In patients with BAV and symptomatic, severe AS, TAVI may be considered AS an alternative to SAVR after consideration of patient-specific procedural risks, values, trade-offs, and preferences, and when the surgery is performed at a Comprehensive Valve Center. ( B-NR, IIb )
Mitral Stenosis
Table 14. Stages of MS
* The transmitral ΔPmean should be obtained to further determine the hemodynamic effect of the MS and is usually >5–10 mm Hg in severe MS. However, due to the variability of the ΔP with heart rate and forward flow, it has not been included in the criteria for severity.
Rheumatic MS
6.2.1.1. Diagnostic Testing: Initial Diagnosis
In patients with signs or symptoms of rheumatic MS, TTE is indicated to establish the diagnosis, quantify hemodynamic severity, assess concomitant valvular lesions, and demonstrate valve morphology (to determine suitability for mitral commissurotomy). ( B-NR, I )
In patients considered for percutaneous mitral balloon commissurotomy (PMBC), TEE should be performed to assess the presence or absence of LA thrombus and to evaluate the severity of MR. ( C-LD, I )
6.2.1.5. Diagnostic Testing: Exercise Testing
In patients with rheumatic MS and a discrepancy between resting echocardiographic findings and clinical symptoms, exercise testing with Doppler or invasive hemodynamic assessment is recommended to evaluate symptomatic response, exercise capacity, and the response of the mean mitral gradient and pulmonary artery pressure. ( C-LD, I )
6.2.2. Medical Therapy
In patients with rheumatic
MS and 1)
AF, 2) a prior embolic event, or 3) an
LA thrombus, anticoagulation with a
VKA is indicated.
( C-LD, I ) In patients with rheumatic MS and AF with a rapid ventricular response, heart rate control can be beneficial. ( C-LD, IIa )
In patients with rheumatic MS in normal sinus rhythm with symptomatic resting or exertional sinus tachycardia, heart rate control can be beneficial to manage symptoms. ( A, IIa )
6.2.3. Intervention
In symptomatic patients (NYHA class II, III, or IV) with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage D) and favorable valve morphology with less than moderate (2+) MR* in the absence of LA thrombus, PMBC is recommended if it can be performed at a Comprehensive Valve Center. ( A, I )
In severely symptomatic patients (NYHA class III or IV) with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage D) who 1) are not candidates for PMBC, 2) have failed a previous PMBC, 3) require other cardiac procedures, or 4) do not have access to PMBC, mitral valve surgery (repair, commissurotomy, or valve replacement) is indicated. ( B-NR, I )
In asymptomatic patients with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage C) and favorable valve morphology with less than 2+ MR in the absence of LA thrombus who have elevated pulmonary pressures (pulmonary artery systolic pressure 50 mm Hg), PMBC is reasonable if it can be performed at a Comprehensive Valve Center. ( B-NR, IIa )
In asymptomatic patients with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage C) and favorable valve morphology with less than 2+ MR* in the absence of LA thrombus who have new onset of AF, PMBC may be considered if it can be performed at a Comprehensive Valve Center. ( C-LD, IIb )
In symptomatic patients (NYHA class II, III, or IV) with rheumatic MS and an mitral valve area >1.5 cm, if there is evidence of hemodynamically significant rheumatic MS on the basis of a pulmonary artery wedge pressure >25 mm Hg or a mean mitral valve gradient >15 mm Hg during exercise, PMBC may be considered if it can be performed at a Comprehensive Valve Center. ( C-LD, IIb )
In severely symptomatic patients (NYHA class III or IV) with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage D) who have a suboptimal valve anatomy and who are not candidates for surgery or are at high risk for surgery, PMBC may be considered if it can be performed at a Comprehensive Valve Center. ( B-NR, IIb )
* 2+ on a 0 to 4+ scale according to Sellar’s criteria or less than moderate by Doppler Echo [Apostolakis EE et al. J Cardiothorac Surg. 2009;4:34].
6.3. Nonrheumatic Calcific MS
In severely symptomatic patients (NYHA class III or IV) with severe MS (mitral valve area ≤1.5 cm±, Stage D) attributable to extensive mitral annular calcification, valve intervention may be considered only after discussion of the high procedural risk and the individual patient’s preferences and values. ( C-LD, IIb )
Figure 7. Intervention for MS

* Repair, commissurotomy, or valve replacement.
Colors correspond to the Class of Recommendation.
Mitral Regurgitation
Table 15. Stages of Chronic Primary MR
* Several valve hemodynamic criteria are provided for assessment of MR severity, but not all criteria for each category will be present in each patient. Categorization of MR severity as mild, moderate, or severe depends on data quality and integration of these parameters in conjunction with other clinical evidence.
7.2.2.1. Diagnostic Testing: Initial Diagnosis
In patients with known or suspected primary MR, TTE is indicated for baseline evaluation of LV size and function, RV function, LA size, pulmonary artery pressure, and the mechanism and severity of primary MR (Stages A to D). ( B-NR, I )
In patients with primary MR, when TTE provides insufficient or discordant information, TEE is indicated for evaluation of the severity of MR, mechanism of MR, and status of LV function (Stages B to D). ( C-EO, I )
In patients with primary MR, CMR is indicated to assess LV and RV volumes and function and may help with assessing MR severity when there is a discrepancy between the findings on clinical assessment and echocardiography. ( B-NR, I )
In patients with severe primary MR undergoing mitral intervention, intraoperative TEE is indicated to establish the anatomic basis for primary MR (Stages C and D) and to guide repair. ( B-NR, I )
7.2.2.2. Diagnostic Testing: Changing Signs or Symptoms
In patients with primary MR (Stages B to D) and new-onset or changing symptoms, TTE is indicated to evaluate the mitral valve apparatus and LV function. ( B-NR, I )
7.2.2.3. Diagnostic Testing: Routine Follow-Up
For asymptomatic patients with severe primary MR (Stages B and C1), TTE is indicated every 6 to 12 months for surveillance of LV function (estimated by LVEF, LVEDD, and LVESD) and assessment of pulmonary artery pressure. ( B-NR, I )
In asymptomatic patients with severe primary MR (Stages B and C1), use of serum biomarkers and novel measurements of LV function, such AS global longitudinal strain, may be considered AS an adjunct to guide timing of intervention. ( B-NR, IIb )
7.2.2.5. Diagnostic Testing: Exercise Testing
In patients with primary MR (Stages B and C) and symptoms that might be attributable to MR, hemodynamic exercise testing using Doppler echocardiography or cardiac catheterization or cardiopulmonary exercise testing is reasonable. ( B-NR, IIa )
7.2.3. Medical Therapy
In symptomatic or asymptomatic patients with severe primary MR and LV systolic dysfunction (Stages C2 and D) in whom surgery is not possible or must be delayed, GDMT for systolic dysfunction is reasonable. ( B-NR, IIa )
In asymptomatic patients with primary MR and normal LV systolic function (Stages B and C1), vasodilator therapy is not indicated if the patient is normotensive. ( B-NR, III (no benefit) )
7.2.4. Intervention
In symptomatic patients with severe primary MR (Stage D), mitral valve intervention is recommended irrespective of LV systolic function. ( B-NR, I )
In asymptomatic patients with severe primary MR and LV systolic dysfunction (LVEF ≤60%, LVESD ≥40 mm) (Stage C2), mitral valve surgery is recommended. ( B-NR, I )
In patients with severe primary MR for whom surgery is indicated, mitral valve repair is recommended in preference to mitral valve replacement when the anatomic cause of MR is degenerative disease, if a successful and durable repair is possible. ( B-NR, I )
In asymptomatic patients with severe primary MR and normal LV systolic function (LVEF ≥60% and LVESD ≤40 mm) (Stage C1), mitral valve repair is reasonable when the likelihood of a successful and durable repair without residual MR is >95% with an expected mortality rate of <1%, when it can be performed at a Primary or Comprehensive Valve Center. ( B-NR, IIa )
In asymptomatic patients with severe primary MR and normal LV systolic function (LVEF >60% and LVESD <40 mm) (Stage C1) but with a progressive increase in LV size or decrease in EF on ≥3 serial imaging studies, mitral valve surgery may be considered irrespective of the probability of a successful and durable repair. ( C-LD, IIb )
In severely symptomatic patients (NYHA class III or IV) with primary severe MR and high or prohibitive surgical risk, transcatheter edge-to-edge repair (TEER) is reasonable if mitral valve anatomy is favorable for the repair procedure and patient life expectancy is at least 1 year. ( B-NR, IIa )
In symptomatic patients with severe primary MR attributable to rheumatic valve disease, mitral valve repair may be considered at a Comprehensive Valve Center by an experienced team when surgical treatment is indicated, if a durable and successful repair is likely. ( B-NR, IIb )
In patients with severe primary MR where leaflet pathology is limited to less than one half the posterior leaflet, mitral valve replacement should not be performed unless mitral valve repair has been attempted at a Primary or Comprehensive Valve Center and was unsuccessful. ( B-NR, III (harm) )
Figure 8. Primary MR

* See Prosthetic Valve section (11.1.2) for choice of mitral valve replacement if mitral valve repair is not possible.
Colors correspond to the Class of Recommendation.
Table 16. Stages of Secondary MR
* Several valve hemodynamic criteria are provided for assessment of MR severity, but not all criteria for each category will be present in each patient. Categorization of MR severity as mild, moderate, or severe depends on data quality and integration of these parameters in conjunction with other clinical evidence.
The measurement of the proximal isovelocity surface area by 2DTTE in patients with secondary MR underestimates the true ERO because of the crescentic shape of the proximal convergence.
‡ May be lower in low-flow states.
7.3.2. Diagnosis of Chronic Secondary MR
In patients with chronic secondary MR (Stages B to D), TTE is useful to establish the etiology and to assess the extent of regional and global LV remodeling and systolic dysfunction, severity of MR, and magnitude of pulmonary hypertension. ( B-NR, I )
In patients with chronic secondary MR (Stages B to D), noninvasive imaging (stress nuclear/PET, CMR, or stress echocardiography), coronary CT angiography, or coronary arteriography is useful to establish etiology of MR and to assess myocardial viability. ( C-EO, I )
In patients with chronic secondary MR with severe symptoms (Stage D) that are unresponsive to GDMT who are being considered for transcatheter mitral valve interventions, TEE is indicated to determine suitability for the procedure. ( B-NR, I )
In patients with chronic secondary MR undergoing transcatheter mitral valve intervention, intraprocedural guidance with TEE is recommended. ( C-EO, I )
7.3.3. Medical Therapy for Secondary MR
In patients with chronic severe secondary MR and HF with reduced LVEF, a cardiologist expert in the management of patients with HF and LV systolic dysfunction should be the primary MDT member responsible for implementing and monitoring optimal GDMT. ( C-EO, I )
7.3.4. Intervention for Secondary MR
In patients with chronic severe secondary MR related to LV systolic dysfunction (LVEF <50%) who have persistent symptoms (NYHA class II, III, or IV) while on optimal GDMT for HF (Stage D), transcatheter edge-to-edge mitral valve (TEER) repair is reasonable in patients with appropriate anatomy AS defined on TEE and with LVEF between 20% and 50%, LVESD ≤70 mm, and pulmonary artery systolic pressure ≤70 mm Hg. ( B-R, IIa )
In patients with severe secondary MR (Stages C and D), mitral valve surgery is reasonable when CABG is undertaken for the treatment of myocardial ischemia. ( B-NR, IIa )
In patients with chronic severe secondary MR from atrial annular dilation with preserved LV systolic function (LVEF ≥50%) who have severe persistent symptoms (NYHA class III or IV) despite therapy for HF and therapy for associated AF or other comorbidities (Stage D), mitral valve surgery may be considered. ( B-NR, IIb )
In patients with chronic severe secondary MR related to LV systolic dysfunction (LVEF <50%) who have persistent severe symptoms (NYHA class III or IV) while on optimal GDMT for HF (Stage D), mitral valve surgery may be considered. ( B-NR, IIb )
In patients with CAD and chronic severe secondary MR related to LV systolic dysfunction (LVEF <50%) (Stage D) who are undergoing mitral valve surgery because of severe symptoms (NYHA class III or IV) that persist despite GDMT for HF, chordal-sparing mitral valve replacement may be reasonable to choose over downsized annuloplasty repair. ( B-R, IIb )
Figure 9. Secondary MR

* Chordal sparing mitral valve replacement may be reasonable to choose over downsided annuloplasty repair.
Colors correspond to the Class of Recommendation.
Table 17. Classification of TR
* Isolated TR is associated with AF and has LVEF >60%, pulmonary artery systolic pressure <50 mm Hg, and no left-sided valve disease, with normal-appearing tricuspid valve leaflets.
Tricuspid Regurgitation
8.2.1. Diagnosis of TR
In patients with TR, TTE is indicated to evaluate the presence and severity of TR, determine the etiology, measure the sizes of the right-sided chambers and inferior vena cava, assess RV systolic function, estimate pulmonary artery systolic pressure, and characterize any associated left-sided heart disease. ( C-LD, I )
In patients with TR, invasive measurement of the cardiac index, right-sided diastolic pressures, pulmonary artery pressures, and pulmonary vascular resistance, AS well AS right ventriculography, can be useful when clinical and noninvasive data are discordant or inadequate. ( C-LD, IIa )
Table 18. Stages of Tricuspid Regurgitation (TR)
8.2.2. Medical Therapy for TR
In patients with signs and symptoms of right-sided HF attributable to severe TR (Stages C and D), diuretics can be useful. ( C-EO, IIa )
In patients with signs and symptoms of right-sided HF attributable to severe secondary TR (Stages C and D), therapies to treat the primary cause of HF (e.g., pulmonary vasodilators to reduce elevated pulmonary artery pressures, GDMT for HF with reduced LVEF, or rhythm control of AF) can be useful. ( C-EO, IIa )
8.2.3. Timing of Intervention
In patients with severe TR (Stages C and D) undergoing left-sided valve surgery, tricuspid valve surgery is recommended. ( B-NR, I )
In patients with progressive TR (Stage B) undergoing left-sided valve surgery, tricuspid valve surgery can be beneficial in the context of either 1) tricuspid annular dilation (tricuspid annulus end diastolic diameter >4.0 cm) or 2) prior signs and symptoms of right-sided HF. ( B-NR, IIa )
In patients with signs and symptoms of right-sided HF and severe primary TR (Stage D), isolated tricuspid valve surgery can be beneficial to reduce symptoms and recurrent hospitalizations. ( B-NR, IIa )
In patients with signs and symptoms of right-sided HF and severe isolated secondary TR attributable to annular dilation (in the absence of pulmonary hypertension or left-sided disease) who are poorly responsive to medical therapy (Stage D), isolated tricuspid valve surgery can be beneficial to reduce symptoms and recurrent hospitalizations. ( B-NR, IIa )
In asymptomatic patients with severe primary TR (Stage C) and progressive RV dilation or systolic dysfunction, isolated tricuspid valve surgery may be considered. ( C-LD, IIb )
In patients with signs and symptoms of right-sided HF and severe TR (Stage D) who have undergone previous left-sided valve surgery, reoperation with isolated tricuspid valve surgery may be considered in the absence of severe pulmonary hypertension or severe RV systolic dysfunction. ( B-NR, IIb )
Figure 10. Tricuspid Regurgitation

Colors correspond to the Class of Recommendation.
9. Pulmonic Valve Disease
See guidelines for the management of adults with congenital heart disease.
Stout KK, et al. Circulation. 2019;139:e698–800.
10. Mixed Valve Disease
10.1. Diagnosis of Mixed VHD
For patients with mixed valve disease, TTE is recommended to assess the etiology, severity, and pathophysiological impact. ( C-EO, I )
In patients with ambiguous symptoms that are suspected to be attributable to mixed mitral valve disease, further assessment of filling pressure by using biomarkers or invasive hemodynamic measurements at rest or with exercise is reasonable. ( C-EO, IIa )
10.1.2. Intervention for Mixed AS and AR
In symptomatic patients with combined AS and AR and a peak transvalvular jet velocity of at least 4.0 m/s or a mean transvalvular gradient of at least 40 mm Hg, AVR is recommended. ( B-NR, I )
In asymptomatic patients with combined AS and AR who have a jet velocity of ≥4.0 m/s with an LVEF <50%, SAVR is recommended. ( C-EO, I )
Table 19. AS/MR Mixed Valve Disease
* Consider TEER as a later staged procedure if symptoms and severe MR persist after treatment of the AS.
11. Prosthetic Valves
11.1.1. Diagnosis and Follow-Up of Prosthetic Valves
In patients with a surgical or transcatheter prosthetic valve and in patients who have had valve repair, an initial postprocedural TTE study is recommended for evaluation of valve hemodynamics and ventricular function. ( B-NR, I )
In patients with a prosthetic valve or prior valve repair and a change in clinical symptoms or signs suggesting valve dysfunction, repeat TTE is recommended. ( C-EO, I )
In patients with a prosthetic valve replacement or prior valve repair and clinical symptoms or signs that suggest prosthetic valve dysfunction, additional imaging with TEE, gated cardiac CT, or fluoroscopy is recommended, even if TTE does not show valve dysfunction. ( C-LD, I )
In patients with a bioprosthetic surgical valve, TTE at 5 and 10 years and then annually after implantation is reasonable, even in the absence of a change in clinical status. ( C-LD, IIa )
In patients with a bioprosthetic TAVI, TTE annually is reasonable. ( C-LD, IIa )
11.1.2. Selection of Prosthetic Valve Type: Bioprosthetic Versus Mechanical Valve
For patients who require heart valve replacement, the choice of prosthetic valve should be based on a shared decision-making process that accounts for the patient’s values and preferences and includes discussion of the indications for and risks of anticoagulant therapy and the potential need for and risks associated with valve reintervention. ( C-LD, I )
For patients of any age requiring valve replacement for whom anticoagulant therapy is contraindicated, cannot be managed appropriately, or is not desired, a bioprosthetic valve is recommended. ( C-EO, I )
For patients <50 years of age who do not have a contraindication to anticoagulation and require AVR, it is reasonable to choose a mechanical aortic prosthesis over a bioprosthetic valve. ( B-NR, IIa )
For patients 50 to 65 years of age who require AVR and who do not have a contraindication to anticoagulation, it is reasonable to individualize the choice of either a mechanical or bioprosthetic AVR, with consideration of individual patient factors and after informed shared decision-making. ( B-NR, IIa )
In patients >65 years of age who require AVR, it is reasonable to choose a bioprosthesis over a mechanical valve. ( B-NR, IIa )
For patients <65 years of age who have an indication for mitral valve replacement, do not have a contraindication to anticoagulation, and are unable to undergo mitral valve repair, it is reasonable to choose a mechanical mitral prosthesis over a bioprosthetic valve. ( B-NR, IIa )
For patients ≥65 years of age who require mitral valve replacement and are unable to undergo mitral valve repair, it is reasonable to choose a bioprosthesis over a mechanical valve. ( B-NR, IIa )
In patients <50 years of age who prefer a bioprosthetic AVR and have appropriate anatomy, replacement of the aortic valve by a pulmonic autograft (the Ross procedure) may be considered at a Comprehensive Valve Center. ( B-NR, IIb )
Table 20. Selected Factors That May Impact Shared Decision-Making for the Choice of Prosthetic Valve
Figure 11. Prosthetic Valves: Choice of Bioprosthetic Versus Mechanical Valve Type

* Approximate ages, based on U.S. Actuarial Life Expectancy tables, are provided for guidance. The balance between expected patient longevity and valve durability varies continuously across the age range, with more durable valves preferred for patients with a longer life expectancy. Bioprosthetic valve durability is finite (with shorter durability for younger patients), whereas mechanical valves are very durable but require lifelong anticoagulation. Long-term (20-y) data on outcomes with surgical bioprosthetic valves are available; robust data on transcatheter bioprosthetic valves extend to only 5 y, leading to uncertainty about longer-term outcomes. The decision about valve type should be individualized on the basis of patient-specific factors that might affect expected longevity.
† See Section 3.2.4.2 for a discussion of the choice of TAVI versus SAVR.
Colors correspond to the Class of Recommendation.
11.2. Antithrombotic Therapy
In patients with a mechanical prosthetic valve, anticoagulation with a
VKA is recommended.
( A, I ) For patients with a mechanical bileaflet or current-generation single-tilting disk
AVR and no risk factors for thromboembolism, anticoagulation with a
VKA to achieve an
INR of 2.5 is recommended.
( B-NR, I ) For patients with a mechanical
AVR and additional risk factors for thromboembolism (e.g.,
AF, previous thromboembolism,
LV dysfunction, hypercoagulable state) or an older-generation prosthesis (e.g., ball-in-cage), anticoagulation with a
VKA is indicated to achieve an
INR of 3.0.
( B-NR, I ) For patients with a mechanical mitral valve replacement, anticoagulation with a
VKA is indicated to achieve an
INR of 3.0.
( B-NR, I ) For patients with a bioprosthetic
TAVI,
aspirin 75 to 100 mg daily is reasonable in the absence of other indications for oral anticoagulants.
( B-R, IIa ) For all patients with a bioprosthetic
SAVR or mitral valve replacement,
aspirin 75 to 100 mg daily is reasonable in the absence of other indications for oral anticoagulants.
( B-NR, IIa ) For patients with a bioprosthetic
SAVR or mitral valve replacement who are at low risk of bleeding, anticoagulation with a
VKA to achieve an
INR of 2.5 is reasonable for at least 3 months and for
AS long
AS 6 months after surgical replacement.
( B-NR, IIa ) For patients with a mechanical
SAVR or mitral valve replacement who are managed with a
VKA and have an indication for antiplatelet therapy, addition of
aspirin 75 to 100 mg daily may be considered when the risk of bleeding is low.
( B-R, IIb ) For patients with a mechanical On-X
AVR and no thromboembolic risk factors, use of a
VKA targeted to a lower
INR (1.5–2.0) may be reasonable starting ≥3 months after surgery, with continuation of
aspirin 75 to 100 mg daily.
( B-R, IIb ) For patients with a bioprosthetic
TAVI who are at low risk of bleeding, dual-antiplatelet therapy with
aspirin 75 to 100 mg and
clopidogrel 75 mg may be reasonable for 3 to 6 months after valve implantation.
( B-NR, IIb ) For patients with a bioprosthetic
TAVI who are at low risk of bleeding, anticoagulation with a
VKA to achieve an
INR of 2.5 may be reasonable for at least 3 months after valve implantation.
( B-NR, IIb ) For patients with bioprosthetic
TAVI, treatment with low-dose
rivaroxaban (10 mg daily) plus
aspirin (75–100 mg) is contraindicated in the absence of other indications for oral anticoagulants.
( B-R, III (harm) ) For patients with a mechanical valve prosthesis, the use of anti-Xa direct oral anticoagulants has not been assessed and is not recommended. ( C-EO, III (harm) )
Figure 12. Antithrombotic Therapy for Prosthetic Valves

* Thromboembolic risk factors include an older-generation valve,
AF, previous thromboembolism, hypercoagulable state, and
LV systolic dysfunction.
For a mechanical On-X
AVR and no thromboembolic risk factors, a goal
INR of 1.5–2.0 plus
aspirin 75–100 mg daily may be reasonable starting ≥3 months after surgery.
Colors correspond to the Class of Recommendation.
11.3. Bridging Therapy During Interruption of Oral Anticoagulation in Patients With Prosthetic Heart Valves
For patients with mechanical heart valves who are undergoing minor procedures (e.g., dental extractions or cataract removal) where bleeding is easily controlled, continuation of
VKA anticoagulation with a therapeutic
INR is recommended.
( C-EO, I ) For patients with a bileaflet mechanical
AVR and no other risk factors for thromboembolism who are undergoing invasive procedures, temporary interruption of
VKA anticoagulation, without bridging agents while the
INR is subtherapeutic, is recommended.
( C-LD, I ) For patients with a mechanical valve prosthesis receiving
VKA therapy who require immediate/emergency noncardiac surgery or an invasive procedure, administration of 4-factor prothrombin complex concentrate (or its activated form) is reasonable.
( C-LD, IIa ) For patients with bioprosthetic heart valves or annuloplasty rings who are receiving anticoagulation for AF, it is reasonable to consider the need for bridging anticoagulant therapy around the time of invasive procedures on the basis of the CHADS2-VASc score weighed against the risk of bleeding. ( C-LD, IIa )
For patients who are undergoing invasive procedures and have 1) a mechanical AVR and any thromboembolic risk factor, 2) an older-generation mechanical AVR, or 3) a mechanical mitral valve replacement, bridging anticoagulation therapy during the preoperative time interval when the INR is subtherapeutic is reasonable on an individualized basis, with the risks of bleeding weighed against the benefits of thromboembolism prevention. ( C-LD, IIa )
11.4. Excessive Anticoagulation and Serious Bleeding With Prosthetic Valves
For patients with mechanical valves and uncontrollable bleeding who require immediate reversal of anticoagulation, administration of 4-factor prothrombin complex (or its activated form) is reasonable. ( C-LD, IIa )
For patients with mechanical valves and uncontrollable bleeding who have received 4-factor prothrombin concentrate complex, adjunctive use of intravenous
vitamin K is reasonable if resumption of
VKA therapy is not anticipated for 7 days.
( C-LD, IIa ) For patients with bioprosthetic valves or annuloplasty rings who are receiving a direct oral anticoagulant and who require immediate reversal of anticoagulation because of uncontrollable bleeding, treatment with idarucizumab (for
dabigatran) or andexanet alfa (for anti-Xa agents) is reasonable.
( B-NR, IIa ) For patients with a mechanical prosthetic valve and supratherapeutic
INR (>5.0) who are not actively bleeding, the benefit of individualized treatment with oral
vitamin K, in addition to temporary withdrawal of the
VKA, is uncertain.
( C-LD, IIb )
11.5. Thromboembolic Events With Prosthetic Valves
In patients with a mechanical
AVR who experience a stroke or systemic embolic event while in therapeutic range on
VKA anticoagulation, it is reasonable to increase the
INR goal from 2.5 (range, 2.0–3.0) to 3.0 (range, 2.5–3.5) or to add daily low-dose
aspirin (75–100 mg), with assessment of bleeding risk.
( C-EO, IIa ) In patients with a mechanical mitral valve replacement who experience a stroke or systemic embolic event while in therapeutic range on
VKA anticoagulation, it is reasonable to increase the
INR goal from 3.0 (range, 2.5–3.5) to 4.0 (range, 3.5–4.0) or to add daily low-dose
aspirin (75–100 mg), with assessment of bleeding risk.
( C-EO, IIa ) In patients with a bioprosthetic surgical or transcatheter aortic valve or bioprosthetic mitral valve who experience a stroke or systemic embolic event while on antiplatelet therapy,
VKA anticoagulation, instead of antiplatelet therapy may be considered after assessment of bleeding risk.
( C-EO, IIb ) Figure 13. Management of Embolic Events and Valve Thrombosis

Colors correspond to the Class of Recommendation.
11.6.1. Diagnosis of Acute Mechanical Valve Thrombosis
In patients with suspected mechanical prosthetic valve thrombosis, urgent evaluation with TTE, TEE, fluoroscopy, and/or multidetector CT imaging is indicated to assess valve function, leaflet motion, and the presence and extent of thrombus. ( B-NR, I )
11.6.2. Intervention for Mechanical Prosthetic Valve Thrombosis
For patients with a thrombosed left-sided mechanical prosthetic heart valve who present with symptoms of valve obstruction, urgent initial treatment with either slow-infusion, low-dose
fibrinolytic therapy or emergency surgery is recommended.
( B-NR, I ) Table 21. Systemic Fibrinolysis Versus Surgery for Prosthetic Valve Thrombosis
11.7.1. Diagnosis of Bioprosthetic Valve Thrombosis
In patients with suspected bioprosthetic valve thrombosis, 3D TEE or 4D CT imaging can be useful to rule out leaflet thrombosis. ( C-LD, IIa )
11.7.2. Medical Therapy
In patients with suspected or confirmed bioprosthetic valve thrombosis who are hemodynamically stable and have no contraindications to anticoagulation, initial treatment with a
VKA is reasonable.
( B-NR, IIa )
11.8.1. Diagnosis of Prosthetic Valve Stenosis
In patients with suspected mechanical or bioprosthetic valve stenosis, TTE and TEE are recommended to diagnosis the cause and severity of valve obstruction, assess ventricular function, and estimate pulmonary artery systolic pressure. ( B-NR, I )
In patients with mechanical valve stenosis, fluoroscopy or cine-CT is recommended to assess motion of the mechanical valve leaflets. ( C-EO, I )
In patients with bioprosthetic valve stenosis, 3D TEE or 4D CT imaging can be useful to rule out leaflet thrombosis. ( C-LD, IIa )
11.8.2. Intervention for Prosthetic Valve Stenosis
In patients with symptomatic severe stenosis of a bioprosthetic or mechanical prosthetic valve, repeat surgical intervention is indicated unless surgical risk is high or prohibitive. ( B-NR, I )
For severely symptomatic patients with bioprosthetic aortic valve stenosis and high or prohibitive surgical risk, a transcatheter ViV procedure is reasonable when performed at a Comprehensive Valve Center. ( B-NR, IIa )
For patients with significant bioprosthetic valve stenosis attributable to suspected or documented valve thrombosis, oral anticoagulation with a
VKA is reasonable.
( B-NR, IIa ) Figure 14. Management of Prosthetic Valve Stenosis and Regurgitation

* See Figure 13 if valve thrombosis is suspected.
Colors correspond to the Class of Recommendation.
11.9.1. Diagnosis of Prosthetic Valve Regurgitation
In patients with suspected mechanical or bioprosthetic valve regurgitation, TTE and TEE are recommended to determine the cause and severity of the leak, assess ventricular function, and estimate pulmonary artery systolic pressure. ( B-NR, I )
In patients undergoing a transcatheter procedure for paravalvular prosthetic regurgitation, 3D TEE is recommended for intraprocedural guidance. ( C-EO, I )
11.9.3. Intervention
In patients with intractable hemolysis or HF attributable to prosthetic transvalvular or paravalvular leak, surgery is recommended unless surgical risk is high or prohibitive. ( B-NR, I )
In asymptomatic patients with severe prosthetic regurgitation and low operative risk, surgery is reasonable. ( B-NR, IIa )
In patients with prosthetic paravalvular regurgitation with the following: 1) either intractable hemolysis or NYHA class III or IV symptoms and 2) who are at high or prohibitive surgical risk and 3) have anatomic features suitable for catheter-based therapy, percutaneous repair of paravalvular leak is reasonable when performed at a Comprehensive Valve Center. ( B-NR, IIa )
For patients with severe HF symptoms caused by bioprosthetic valve regurgitation who are at high to prohibitive surgical risk, a transcatheter ViV procedure is reasonable when performed at a Comprehensive Valve Center. ( B-NR, IIa )
12. Infective Endocarditis
12.2. Diagnosis of IE
In patients at risk of IE (e.g., those with congenital or acquired VHD, previous IE, prosthetic heart valves, certain congenital or heritable heart malformations, immunodeficiency states, or injection drug use) who have unexplained fever blood, culture samples should be obtained. ( B-NR, I )
In patients with the recent onset of left-sided valve regurgitation, at least 2 sets of blood culture samples should be obtained. ( B-NR, I )
In patients with suspected IE, the Modified Duke Criteria should be used for diagnosis (Tables 20 and 21). ( B-NR, I )
Patients with IE should be evaluated and managed with consultation with a multispecialty Heart Valve Team, which includes an infectious disease specialist, cardiologist, and cardiac surgeon; a cardiac anesthesiologist for surgically managed patients (11); and a neurologist for patients with neurological events. ( B-NR, I )
In patients with suspected IE, TTE is recommended to identify vegetations, characterize the hemodynamic severity of valvular lesions, assess ventricular function and pulmonary pressures, and detect complications. ( B-NR, I )
In all patients with known or suspected IE and nondiagnostic TTE results, when complications have developed or are clinically suspected or when intracardiac device leads are present, TEE is recommended. ( B-NR, I )
In patients with IE who have a change in clinical signs or symptoms (e.g., new murmur, embolism, persistent fever, HF, abscess, or atrioventricular heart block) and in patients at high risk of complications (e.g., extensive infected tissue, large vegetation on initial echocardiogram, or staphylococcal, enterococcal, or fungal infections), TTE and/or TEE are recommended for reevaluation. ( B-NR, I )
In patients undergoing valve surgery for IE, intraoperative TEE is recommended. ( B-NR, I )
In patients being considered for an early change to oral antibiotic therapy for the treatment of stable IE, a baseline TEE before switching to oral therapy and a repeat TEE 1 to 3 days before completion of the oral antibiotic regimen should be performed. ( B-NR, I )
In patients with Staphylococcus aureus bacteremia without a known source, TEE is reasonable to diagnose possible IE. ( B-NR, IIa )
In patients with a prosthetic valve in the presence of persistent fever without bacteremia or a new murmur, a TEE is reasonable to aid in the diagnosis of IE. ( B-NR, IIa )
In patients in whom the anatomy cannot be clearly delineated by echocardiography in the setting of suspected paravalvular infections, CT imaging is reasonable. ( B-NR, IIa )
In patients classified by Modified Duke Criteria AS having “possible IE,” 18F-fluorodeoxyglucose PET/CT is reasonable AS adjunct diagnostic imaging. ( B-NR, IIa )
In patients with nosocomial S. aureus bacteremia with a known portal of entry from an extracardiac source, TEE might be considered to detect concomitant staphylococcal IE. ( B-NR, IIb )
Figure 15. Diagnosis of IE

Colors correspond to the Class of Recommendation.
Table 22. Diagnosis of IE According to the Proposed Modified Duke Criteria
Table 23. Major and Minor Criteria in the Modified Duke Criteria for the Diagnosis of IE
* Excludes single positive cultures for coagulase-negative staphylococci and organisms that do not cause IE.
12.3. Medical Therapy for IE
In patients with IE, appropriate antibiotic therapy should be initiated and continued after blood cultures are obtained, with guidance from antibiotic sensitivity data and the infectious disease experts on the MDT. ( B-NR, I )
Patients with suspected or confirmed IE associated with drug use should be referred to addiction treatment for opioid substitution therapy. ( B-R, I )
In patients with IE and with evidence of cerebral embolism or stroke, regardless of the other indications for anticoagulation, it is reasonable to temporarily discontinue anticoagulation. ( B-NR, IIa )
In patients with IE and with evidence of cerebral embolism or stroke, regardless of the other indications for anticoagulation, it is reasonable to temporarily discontinue anticoagulation. ( B-NR, IIa )
In patients with left-sided IE caused by streptococcus, Enterococcus faecalis, S. aureus, or coagulase-negative staphylococci deemed stable by the MDT after initial intravenous antibiotics, a change to oral antibiotic therapy may be considered if TEE before the switch to oral therapy shows no paravalvular infection, if frequent and appropriate follow-up can be assured by the care team, and if a follow-up TEE can be performed 1 to 3 days before the completion of the antibiotic course. ( B-R, IIb )
In patients receiving
VKA anticoagulation at the time of
IE diagnosis, temporary discontinuation of
VKA anticoagulation may be considered.
( B-NR, IIb ) Patients with known VHD should not receive antibiotics before blood cultures are obtained for unexplained fever. ( C-LD, III (harm) )
12.4. Intervention for IE
Decisions about the timing of surgical intervention for IE should be made by a Heart Valve Team. ( B-NR, I )
In patients with IE who present with valve dysfunction resulting in symptoms of HF, early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) is indicated. ( B-NR, I )
In patients with left-sided IE caused by S. aureus, a fungal organism, or other highly resistant organisms, early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) is indicated. ( B-NR, I )
In patients with IE complicated by heart block, annular or aortic abscess, or destructive penetrating lesions, early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) is indicated. ( B-NR, I )
In patients with IE and evidence of persistent infection AS manifested by persistent bacteremia or fevers lasting >5 days after onset of appropriate antimicrobial therapy, early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) for IE is indicated. ( B-NR, I )
In all patients with definite endocarditis and an implanted cardiac electronic device, complete removal of the pacemaker or defibrillator systems, including all leads and the generator, is indicated. ( B-NR, I )
For patients with prosthetic valve endocarditis and relapsing infection (defined AS recurrence of bacteremia after a complete course of appropriate antibiotics and subsequent negative blood culture results) without other identifiable source of infection, surgery is recommended. ( C-LD, I )
In patients with recurrent endocarditis and continued intravenous drug use, consultation with addiction medicine is recommended to discuss the long-term prognosis for the patient’s refraining from actions that risk reinfection before repeat surgical intervention is considered. ( C-LD, I )
In patients with IE who present with recurrent emboli and persistent vegetations despite appropriate antibiotic therapy, early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) is reasonable. ( B-NR, IIa )
In patients with native left-sided valve endocarditis who exhibit mobile vegetations >10 mm in length (with or without clinical evidence of embolic phenomenon), early surgery (during initial hospitalization and before completion of a full therapeutic course of antibiotics) may be considered. ( B-NR, IIb )
In patients with IE and an indication for surgery who have suffered a stroke but have no evidence of intracranial hemorrhage or extensive neurological damage, operation without delay may be considered. ( B-NR, IIb )
For patients with IE and major ischemic stroke with extensive neurological damage or intracranial hemorrhage, if the patient is hemodynamically stable, delaying valve surgery for at least 4 weeks may be considered. ( B-NR, IIb )
Figure 16. Endocarditis Treatment

* IE caused by streptococcus, Enterococcus faecalis, Staphylococcus aureus, or coagulase-negative staphylococci deemed stable by the Heart Valve Team.
† Early surgery defined as during initial hospital course and before completion of a full course of appropriate antibiotics.
13. Pregnancy and VHD
13.1. Initial Management of Women With VHD Before and During Pregnancy
Women with suspected valve disease who are considering pregnancy should undergo a clinical evaluation and TTE before pregnancy. ( B-NR, I )
Women with severe valve disease (Stages C and D) who are considering pregnancy should undergo pre-pregnancy counseling by a cardiologist with expertise in managing women with VHD during pregnancy. ( B-NR, I )
Pregnant women with severe valve disease (Stages C and D) should be monitored in a tertiary-care center with a dedicated Heart Valve Team of cardiologists, surgeons, anesthesiologists, and maternal-fetal medicine obstetricians with expertise in the management of high-risk cardiac conditions during pregnancy. ( B-NR, I )
In asymptomatic women with severe valve disease (Stage C1) who are considering pregnancy, exercise testing is reasonable before pregnancy for risk assessment. ( B-NR, IIa )
13.1.1. Medical Therapy for Women With VHD Before and During Pregnancy
In pregnant women with VHD, beta-blocker medications are reasonable AS required for heart rate control or treatment of arrhythmias. ( C-LD, IIa )
In pregnant women with VHD and HF symptoms (Stage D), diuretic medications are reasonable if needed for volume overload. ( C-LD, IIa )
In pregnant women with
VHD,
ACE inhibitors and ARBs should not be given because of fetal risk.
( B-NR, III (harm) )
13.1.2. Intervention for Women With Native VHD Before and During Pregnancy
In symptomatic women with severe VHD who are considering pregnancy, intervention before pregnancy is recommended on the basis of standard indications. ( B-NR, I )
In women who require a valve intervention before pregnancy, the choice of prosthetic valve should be based on a shared decision-making process that accounts for the patient’s values and preferences, including discussion of the risks of mechanical valves during pregnancy and the reduced durability of bioprosthetic valves in young women. ( C-EO, I )
In asymptomatic women with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage C1) who are considering pregnancy, PMBC at a Comprehensive Valve Center is reasonable before pregnancy for those who have favorable valve morphology. ( C-LD, IIa )
In women of childbearing age who require valve replacement, bioprosthetic valves are preferred over mechanical valves because of the increased maternal and fetal risks of mechanical heart valves in pregnancy. ( B-NR, IIa )
In asymptomatic women with severe AS (aortic velocity ≥4.0 m/s or mean pressure gradient ≥40 mm Hg, Stage C) who are considering pregnancy, valve intervention before pregnancy is reasonable. ( C-EO, IIa )
In asymptomatic women with severe AS (aortic velocity ≥4.0 m/s or mean pressure gradient ≥40 mm Hg, Stage C1) who are considering pregnancy, do not meet COR 1 criteria for intervention, and have a preconception evaluation confirming the absence of symptoms (including normal exercise stress testing and serum BNP measurements), medical management during pregnancy may be considered to avoid prosthetic valve replacement. ( C-EO, IIb )
In asymptomatic women with severe MR (Stage C1) and a valve suitable for repair who are considering pregnancy, valve repair before pregnancy at a Comprehensive Valve Center may be considered but only after detailed discussion with the patient about the risks and benefits of the surgery and its effect on future pregnancies. ( C-EO, IIb )
Figure 17. Preconception Management of Women with Native Valve Disease

Colors correspond to the Class of Recommendation.
13.1.2.2. During-Pregnancy Intervention
In pregnant women with severe AS (mean pressure gradient ≥40 mm Hg, Stage D), valve intervention during pregnancy is reasonable if there is hemodynamic deterioration or if there are NYHA class III or IV HF symptoms. ( B-NR, IIa )
In pregnant women with severe rheumatic MS (mitral valve area ≤1.5 cm, Stage D) and with valve morphology favorable for PMBC who remain symptomatic with NYHA class III or IV HF symptoms despite medical therapy, PMBC is reasonable during pregnancy if it is performed at a Comprehensive Valve Center. ( B-NR, IIa )
In pregnant women with severe valve regurgitation and with NYHA class IV HF symptoms (Stage D) refractory to medical therapy, valve surgery is reasonable during pregnancy. ( C-LD, IIa )
In pregnant women with VHD, valve surgeries should not be performed in the absence of severe HF symptoms refractory to medical therapy. ( C-LD, III (harm) )
13.2.1. Initial Management of Prosthetic Heart Valves in Pregnant Women
Women with a prosthetic valve should undergo pre-pregnancy assessment, including echocardiography, by a cardiologist with expertise in managing women with VHD during pregnancy. ( C-EO, I )
Pregnant women with a mechanical prosthesis should be monitored in a tertiary-care center with a dedicated MDT of cardiologists, surgeons, anesthesiologists, and maternal-fetal medicine obstetricians with expertise in the management of high-risk cardiac conditions during pregnancy. ( C-EO, I )
Women with mechanical heart valves considering pregnancy should be counselled that pregnancy is high risk and that there is no anticoagulation strategy that is consistently safe for the mother and baby. ( B-NR, I )
Pregnant women with a mechanical prosthetic valve who have prosthetic valve obstruction or experience an embolic event should undergo a TEE. ( B-NR, I )
13.2.2. Anticoagulation for Pregnant Women With Mechanical Prosthetic Heart Valves
Pregnant women with mechanical prostheses should receive therapeutic anticoagulation with frequent monitoring during pregnancy. ( B-NR, I )
Women with mechanical heart valves who cannot maintain therapeutic anticoagulation with frequent monitoring should be counseled against pregnancy. ( B-NR, I )
Women with mechanical heart valves and their providers should use shared decision-making to choose an anticoagulation strategy for pregnancy. Women should be informed that
VKA during pregnancy is associated with the lowest likelihood of maternal complications but the highest likelihood of miscarriage, fetal death, and congenital abnormalities, particularly if taken during the first trimester and if the
warfarin dose exceeds 5 mg/d.
( B-NR, I ) Pregnant women with mechanical valve prostheses who are on
warfarin should switch to twice-daily
LMWH (with a target anti-Xa level of 0.8 U/mL to 1.2 U/mL at 4 to 6 hours after dose) or intravenous
UFH (with an activated partial thromboplastin time [
aPTT] 2 times control) at least 1 week before planned delivery.
( C-LD, I ) Pregnant women with mechanical valve prostheses who are on
LMWH should switch to
UFH (with an
aPTT 2 times control) at least 36 hours before planned delivery.
( C-LD, I ) Pregnant women with valve prostheses should stop
UFH at least 6 hours before planned vaginal delivery.
( C-LD, I ) If labor begins or urgent delivery is required in a woman therapeutically anticoagulated with a
VKA, cesarean section should be performed after reversal of anticoagulation.
( C-LD, I ) For pregnant women with mechanical prostheses who require a dose of
warfarin ≤5 mg/d to maintain a therapeutic
INR, continuation of
warfarin for all 3 trimesters is reasonable after full discussion with the patient about risks and benefits.
( B-NR, IIa ) For pregnant women with mechanical prostheses who require >5 mg/d of
warfarin to achieve a therapeutic
INR, dose-adjusted
LMWH (with a target anti-Xa level of 0.8 to 1.2 U/mL at 4 to 6 hours after dose) at least 2 times per day during the first trimester, followed by
warfarin during the second and third trimesters, is reasonable.
( B-NR, IIa ) For pregnant women with mechanical prostheses who require a dose of
warfarin >5 mg/d to achieve a therapeutic
INR, and for whom dose-adjusted
LMWH is unavailable, dose-adjusted continuous intravenous
UFH during the first trimester (with
aPTT 2 times control), followed by
warfarin for the second and third trimesters, is reasonable.
( B-NR, IIa ) For hemodynamically stable pregnant women with obstructive left-sided mechanical valve thrombosis, it is reasonable to manage with slow-infusion, low-dose
fibrinolytic therapy.
( B-NR, IIa ) For pregnant women with mechanical prostheses who require a
warfarin dose >5 mg/d to achieve a therapeutic
INR, dose-adjusted
LMWH (with a target anti-Xa level of 0.8 to 1.2 U/mL at 4 to 6 hours after dose) at least 2 times per day for all 3 trimesters may be considered.
( B-NR, IIb ) For pregnant women with mechanical prostheses who require a dose of
warfarin ≤5 mg/d to maintain a therapeutic
INR, dose-adjusted
LMWH at least 2 times per day during the first trimester, followed by
warfarin for the second and third trimesters, may be considered.
( B-NR, IIb ) For pregnant women with mechanical prostheses,
aspirin 75 to 100 mg daily may be considered, in addition to anticoagulation, if needed for other indications.
( B-NR, IIb ) For pregnant women with mechanical prostheses,
LMWH should not be administered unless anti-Xa levels are monitored 4 to 6 hours after administration and dose is adjusted according to levels.
( B-NR, III (harm) ) The use of anti-Xa direct oral anticoagulants with mechanical heart valves in pregnancy has not been assessed and is not recommended. ( C-EO, III (harm) )
Figure 18. Anticoagulation for Prosthetic Mechanical Heart Valves in Women During Pregnancy

* Dose-adjusted LMWH should be given at least 2 times per day, with close monitoring of anti-Xa levels. Target to Xa level of 0.8 to 1.2 U/mL, 4 to 6 hours after dose. Trough levels may aid in maintaining patient in therapeutic range. Continuous UFH should be adjusted to aPTT 2 times control.
Colors correspond to the Class of Recommendation.
14. Surgical Considerations
14.1.1. Management of CAD in Patients Undergoing TAVI
In patients undergoing TAVI, 1) contrast-enhanced coronary CT angiography (in patients with a low pretest probability for CAD) or 2) an invasive coronary angiogram is recommended to assess coronary anatomy and guide revascularization. ( C-EO, I )
In patients undergoing TAVI with significant left main or proximal CAD with or without angina, revascularization by PCI before TAVI is reasonable. ( C-LD, IIa )
In patients with significant AS and significant CAD (luminal reduction >70% diameter, fractional flow reserve <0.8, instantaneous wave-free ratio <0.89) consisting of complex bifurcation left main and/or multivessel CAD with a SYNTAX (Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery) score >33, SAVR and CABG are reasonable and preferred over TAVI and PCI. ( C-LD, IIa )
14.1.2. Management of CAD in Patients Undergoing Valve Surgery
In patients with symptoms of angina, objective evidence of ischemia, decreased LV systolic function, history of CAD, or coronary risk factors (including men >40 years of age and postmenopausal women), invasive coronary angiography is indicated before valve intervention. ( C-LD, I )
In patients with chronic severe secondary MR, invasive coronary angiography should be performed AS part of the evaluation. ( C-LD, I )
In selected patients with a low to intermediate pretest probability of CAD, contrast-enhanced coronary CT angiography is reasonable to exclude the presence of significant obstructive CAD. ( B-NR, IIa )
In patients undergoing valve repair or replacement with significant proximal CAD (≥70% reduction in luminal diameter in major coronary arteries or ≥50% reduction in luminal diameter in the left main coronary artery and/or physiologically significance), CABG is reasonable for selective patients. ( C-LD, IIa )
14.2. Intervention for AF in Patients With VHD
In patients with VHD and AF for whom surgical intervention is planned, the potential symptomatic benefits and additional procedural risks of adjunctive arrhythmia surgery at the time of cardiac valvular surgery should be discussed with the patient. ( C-LD, I )
For symptomatic patients with paroxysmal or persistent AF who are undergoing valvular surgery, surgical pulmonary vein isolation or a maze procedure can be beneficial to reduce symptoms and prevent recurrent arrhythmias. ( B-R, IIa )
For patients with AF or atrial flutter who are undergoing valve surgery, LA appendage ligation/excision is reasonable to reduce the risk of thromboembolic events. ( B-NR, IIa )
In patients undergoing LA surgical ablation of atrial arrhythmias and/or LA appendage ligation/excision, anticoagulation therapy is reasonable for at least 3 months after the procedure. ( B-NR, IIa )
For patients without atrial arrhythmias who are undergoing valvular surgery, LA appendage occlusion/exclusion/amputation is potentially harmful. ( B-NR, III (harm) )
Figure 19. Management of CAD in Patients Undergoing Valve Interventions

* Including men age >40 years and postmenopausal women.
Colors correspond to the Class of Recommendation.
Figure 20. Intervention for AF in Patients With VHD

Colors correspond to the Class of Recommendation.
15. Noncardiac Surgery in Patients With VHD
15.1. Diagnosis of Patients With VHD Undergoing Noncardiac Surgery
In patients with clinically suspected moderate or greater degrees of valvular stenosis or regurgitation who are undergoing noncardiac surgery, preoperative echocardiography is recommended. ( C-EO, I )
15.2. Management of the Symptomatic Patient With VHD Undergoing Noncardiac Surgery
In patients who meet standard indications for intervention for VHD (replacement and repair) on the basis of symptoms and disease severity, intervention should be performed before elective noncardiac surgery to reduce perioperative risk if possible, depending on the urgency and risk of the noncardiac procedure. ( C-EO, I )
15.3. Management of the Asymptomatic Patient With VHD Undergoing Noncardiac Surgery
In asymptomatic patients with moderate or greater degrees of AS and normal LV systolic function, it is reasonable to perform elective noncardiac surgery. ( B-R, IIa )
In asymptomatic patients with moderate or greater degrees of rheumatic MS with less than severe pulmonary hypertension (pulmonary artery systolic pressure <50 mm Hg), it is reasonable to perform elective noncardiac surgery. ( C-EO, IIa )
In asymptomatic patients with moderate or greater degrees of MR and normal LV systolic function with less than severe pulmonary hypertension (pulmonary artery systolic pressure <50 mm Hg), it is reasonable to perform elective noncardiac surgery. ( C-LD, IIa )
In asymptomatic patients with moderate or greater degrees of AR and normal LV systolic function, it is reasonable to perform elective noncardiac surgery. ( C-LD, IIa )
Class of Recommendations and Level of Evidence
COR and LOE are determined independently (any COR may be paired with any LOE).
A recommendation with LOE C does not imply that the recommendation is weak. Many important clinical questions addressed in guidelines do not lend themselves to clinical trials. Although RCTs are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
* The outcome or result of the intervention should be specified (an improved clinical outcome or increased diagnostic accuracy or incremental prognostic information).
† For comparative-effectiveness recommendations (COR I and IIa; LOE A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
‡ The method of assessing quality is evolving, including the application of standardized, widely used, and preferably validated evidence grading tools; and for systematic reviews, the incorporation of an Evidence Review Committee.
COR indicates Class of Recommendation; EO, expert opinion; LD, limited data; LOE, Level of Evidence; NR, nonrandomized; R, randomized; RCT, randomized controlled trial.
Abbreviations
- 2D
- 2-dimensional
- 3D
- 3-dimensional
- ACE
- angiotensin-converting enzyme
- AF
- atrial fibrillation
- aPTT
- activated partial thromboplastin time
- AR
- aortic regurgitation
- ARB
- angiotensin receptor blocker
- AS
- aortic stenosis
- ASA
- aspirin
- AVA
- aortic valve area
- AVAi
- aortic valve area indexed to body surface area
- AVR
- aortic valve replacement
- BAV
- bicuspid aortic valve
- BID
- two times a day
- BNP
- B-type natriuretic peptide
- BP
- blood pressure
- CABG
- coronary artery bypass graft
- CAD
- coronary artery disease
- CKD
- chronic kidney disease
- CMR
- cardiac magnetic resonance
- CNS
- central nervous system
- COR
- Class of Recommendation
- CRT
- cardiac resynchronization therapy
- CT
- computed tomography
- CW
- continuous wave
- DLCO2
- diffusion capacity for carbon dioxide
- DOAC
- direct oral anticoagulants
- DSE
- dobutamine stress echocardiography
- ECG
- electrocardiogram
- EF
- ejection fraction
- ERO
- effective regurgitant orifice
- ETT
- exercise treadmill test
- FEV1
- forced expiratory volume in 1 second
- GDMT
- guideline determined medical therapy
- GI
- gastrointestinal
- HF
- heart failure
- ICD
- implantable cardioverter defibrillator
- IE
- infective endocarditis
- INR
- international normalized ratio
- IV
- intravenous
- IVC
- inferior vena cava
- LA
- left atrium
- LMWH
- low molecular weight heparin
- LOE
- Level of Evidence
- LV
- left ventricle
- LVEDD
- left ventricular end-diastolic dimension
- LVEF
- left ventricular ejection fraction
- LVESD
- left ventricular end-systolic dimension
- LVOT
- left ventricular outflow tract
- MDT
- multidisciplinary team
- MI
- myocardial infarction
- MR
- mitral regurgitation
- MS
- mitral stenosis
- MV
- mitral valve
- MVA
- mitral valve area
- MVR
- mitral valve replacement
- NOAC
- non–vitamin K oral anticoagulant
- NVE
- native valve endocarditis
- NYHA
- New York Heart Association
- PA
- pulmonary artery
- PASP
- pulmonary artery systolic pressure
- PCI
- non–vitamin K oral anticoagulant
- PET
- positron emission tomography
- PHTN
- pulmonary hypertension
- PMBC
- percutaneous mitral balloon commissurotomy
- PO
- by mouth
- PR
- pulmonic regurgitation
- PROM
- predicted risk of mortality
- PVE
- prosthetic valve endocarditis
- QD
- once daily
- RA
- right atrium
- RCT
- randomized controlled trial
- RF
- regurgitant fraction
- RV
- right ventricular
- RVH
- right ventricular hypertrophy
- RVol
- regurgitant volume
- RVOT
- right ventricular outflow tract
- Rx
- therapy
- S. aureus
- Staphylococcus aureus
- SAVR
- surgical aortic valve replacement
- SC
- subcutaneous
- spp
- species
- STS
- Society of Thoracic Surgeons
- T 1/2
- half-life
- TA
- tricuspid annular
- TAVI
- transcatheter aortic valve implantation
- TAVR
- transcatheter aortic valve replacement
- TEE
- transesophageal echocardiography
- TEER
- transcatheter aortic valve implantation
- TR
- tricuspid regurgitation
- TS
- tricuspid stenosis
- TTE
- transthoracic echocardiography/echocardiogram
- TV
- tricuspid valve
- TVR
- tricuspid valve replacement
- UFH
- unfractionated heparin
- V max
- maximal velocity
- VHD
- valvular heart disease
- VKA
- vitamin K antagonist
- ΔP
- pressure gradient
Source Citation
Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O'Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2;143(5):e72-e227. doi: 10.1161/CIR.0000000000000923. Epub 2020 Dec 17. Erratum in: Circulation. 2021 Feb 2;143(5):e229. PMID: 33332150.
Disclaimer
This resource is for informational purposes only, intended as a quick-reference tool based on the cited source guideline(s), and should not be used as a substitute for the independent professional judgment of healthcare providers. Practice guidelines are unable to account for every individual variation among patients or take the place of clinician judgment, and the ultimate decision concerning the propriety of any course of conduct must be made by healthcare providers after consideration of each individual patient situation. Guideline Central does not endorse any specific guideline(s) or guideline recommendations and has not independently verified the accuracy hereof. Any use of this resource or any other Guideline Central resources is strictly voluntary.

