Design and created by Guideline Central in participation with the American Society of Addiction Medicine.
Opioid Addiction Treatment Patient Guide
A Guide for Patients, Families and Friends
Updated for 2025
American Society of Addiction Medicine
Publication Date: June 12, 2025
INTRODUCTION
DEFINITION OF ADDICTION*
ASSESSMENT
Getting Started
- The clinician will ask questions to understand all of the factors that contribute to the patient’s addiction. The more that is known, the better treatment can be planned with the patient. The patient will likely be asked about:
- Current drug and alcohol use
- Withdrawal symptoms
- History of substance use
- Family history of addiction
- Mental or physical health problems
- Support systems
- Access to safe, stable housing
- Motivation to change
- The next step is a complete examination to check the patient’s overall physical and mental health. This includes finding other common conditions related to addiction that may impact the plan for treatment.
- The physical examination will often include a drug test.
TREATMENT OVERVIEW
During the assessment, the clinician will also identify the patient’s psychological and social support needs. They will likely recommend counseling or recovery support services, such as mutual support group participation. However, participation in counseling and other support services should not be required to receive treatment with medication. If the patient does participate in mutual support groups it is important to find a group that issupportive of the use of medications for opioid use disorder.
While a comprehensive assessment and medical evaluation are important for developing a treatment plan, completion of all assessments should not delay or prevent the patient from starting medication.
After the assessment, the clinician will discuss all recommended treatment options with the patient. Every patient situation is different, so choosing the best options is a shared decision between the patient and the clinician.
There are three main choices for medication to treat opioid addiction: methadone, buprenorphine, and naltrexone. These medications are typically recommended in combination with counseling and other support services.
- ASAM Level 1 - Outpatient treatment. For example, medication treatment with a primary care provider.
- ASAM Level 2 - Intensive outpatient or high intensity outpatient. In an intensive outpatient program, the patient receives 9–19 hours per week of treatment services. In high intensity outpatient, patients receive over 20 hours of treatment services per week.
- ASAM Level 3 - Residential treatment. Residential treatment programs provide treatment in a safe, homelike setting where the patient can practice skills needed for recovery.
- ASAM Level 4 - Medically managed inpatient treatment. Inpatient treatment may be needed for patients with severe medical or psychiatric problems that require medical and nurse care.
Treatment Plan
- After discussing the assessment results and treatment choices with the clinician, it’s time to develop the full treatment plan.
This can include:- Treatment goals
- Medications: usually methadone, buprenorphine or naltrexone for opioid use disorder
- Treatment schedule
- Counseling plan
- Recovery support services
- What to expect in the next phase of treatment
- A safety plan
Patient Participation
- Patient engagement in treatment and recovery improves outcomes. Treatment should be long term, since addiction is a chronic disease. For this reason, it is important that patients work with clinicians to develop a treatment plan that is tailored to their needs and goals.
- Patients should expect to be treated with respect and dignity and have their concerns listened to when starting or changing the treatment plan.
- To avoid health problems, patients must let their clinicians know about any other medications they are taking or if they drink alcohol. This is very important — certain medications and alcohol can cause major problems when combined with treatment medications.
- Common patient responsibilities include:
- Keeping all appointments
- Providing samples for drug testing
- Taking medications as prescribed
- Allowing and encouraging involvement of supportive family and friends
- Avoiding persons, places and situations that may put them at risk of relapse.
Counseling
- Counseling is an important part of treatment for many patients and is usually recommended with medications.
- Counseling should be provided by a qualified clinician. Patients may receive counseling in the same place where they receive medication or in another location.
- Counseling helps patients address personal, social or other problems that may contribute to their addiction. Examples can be:
- Increasing motivation for treatment and recovery
- Difficult situations at work or home
- Building a support system of people who are supportive of recovery
- All of the clinicians involved in patient treatment should work together to coordinate care.
- In addition to counseling, patients are encouraged to join support groups that include others who are also in recovery.
- Counseling and support groups are not limited to the patient. There are also many counseling services and support groups for family and friends of those dealing with addiction. Remember, addiction affects friends and family as well.
Support from Family and Friends
- Families and friends can play a key role in supporting their loved ones to achieve a long-lasting recovery.
- It is very important that patients avoid the people, places and other things that trigger their desire to use alcohol or drugs. They also need to learn how to respond to those triggers without using alcohol or drugs. Friends and family can provide support and encouragement throughout this process.
WITHDRAWAL
- Opioid withdrawal refers to the wide range of painful and unpleasant symptoms (such as vomiting, diarrhea, and muscle pain) that occur after stopping or cutting down on the use of opioids. Withdrawal can last more than 10 days but is most often between 3–5 days.
- While rare, opioid withdrawal can be life threatening.
- Using medications to control withdrawal (also called withdrawal management) is almost always recommended over trying to endure withdrawal without treatment. When patients do try to stop using opioids without treatment it can lead to stronger cravings and continued use.
- Withdrawal management on its own is not a treatment for opioid addiction and may increase the risk of relapse, overdose, and overdose death.
- Methadone and buprenorphine can treat both opioid withdrawal and opioid addiction and are usually recommended.
- Lofexidine and clonidine are safe and effective for management of opioid withdrawal, but methadone and buprenorphine are more effective.
- Opioid withdrawal management using ultra-rapid opioid detoxification (UROD) is NOT recommended due to high risk for adverse events including death.
MEDICATIONS TO TREAT OPIOID ADDICTION
Medications To Treat Opioid Addiction
| Medication | Brand Names |
|---|---|
| Buprenorphine | Sublocade® (Injection), Brixadi® (injection), generics (films or tablets) |
| Buprenorphine and naloxone | Bunavail®, Cassipa®, Suboxone®, Zubsolv®, generics (films or tablets) |
| Methadone | generics (liquid or tablets to dissolve in water) |
| Extended release naltrexone | Vivitrol® (injection) |
OPIOID ADDICTION MEDICATION
- All FDA-approved medications—including methadone, buprenorphine and naltrexone—for the treatment of opioid use disorder should be available to all patients.
- Counseling is recommended with the use of any of these medications. However, counseling should not be required in order to receive treatment with medication.
- Patient preferences, history, and illness severity should all be considered when deciding which medication is best for each patient.
- Each medication works in a different way and has its own risks and benefits. Once started, these medications can be safely taken for years. The clinician and the patient should review together the risks and benefits of each medication.
- When used properly, these medications help restore balance to the parts of the brain that are impacted by addiction, helping patients to manage their addiction so they can recover.
- There is no typical timeline for use of medication. It differs for each patient. Some patients may need medications for many years.
- Some people have special situations such as pregnancy, mental health issues, pain, or criminal justice system involvement. They should discuss these issues with their clinician to find the right medication for their needs.
- Adolescents and their caregivers should also discuss medication options with their clinicians.
Buprenorphine
- Buprenorphine acts on the same parts of the brain as opioid medications or drugs. It helps to stabilize them to reduce the desire to use opioids and to prevent withdrawal symptoms.
- There are several buprenorphine formulations approved by the FDA for treatment of opioid use disorder.
- Buprenorphine comes as tablets or films (for daily use) or extended-release injections (weekly or monthly). The dosage may be adjusted over time to find the dose that works best for the patient.
- Many versions of this medication are combined with naloxone to prevent possible misuse. When misused (injected, snorted, or other) the naloxone in the buprenorphine medication can bring on withdrawal symptoms.
- Insurance coverage and price may help determine which form should be chosen. The clinician will make sure the patient has a dosage and form that meets their medical needs.
- Patients may need to see their clinician frequently at the beginning of treatment, until their addiction symptoms have stabilized.
- Buprenorphine treatment can be started either at home or in a doctor’s office. Both options are considered safe and effective when starting.
- Buprenorphine needs to be started carefully to prevent withdrawal symptoms. The clinician may ask the patient to wait until they are experiencing mild to moderate opioid withdrawal symptoms before taking the first dose of buprenorphine.
- Many patients will need to continue taking buprenorphine for an extended period of time. Stopping buprenorphine can put the patient at risk for relapse and overdose. This should only be done slowly with careful monitoring by the clinician.
- As of 2023, any clinician with a current DEA registration that includes Schedule III authority may now prescribe buprenorphine. This significantly increases the number of clinicians eligible to prescribe buprenorphine, and provides patients with easier access to effective treatments.
- Treatment with buprenorphine has been shown to reduce the patient’s risk for opioid overdose death.
Methadone
- Methadone also acts on the same part of the brain as opioid medications or drugs. It helps to stabilize them to reduce the desire to use opioids and to prevent withdrawal symptoms.
- Methadone can be safely started before the patient starts to experience withdrawal symptoms.
- The clinician will work closely with the patient to find the right dose that reduces cravings without causing the patient to feel drowsy or overtired.
- Methadone comes as a liquid, or as a powder or tablet that is dissolved in liquid before it is taken. It is typically taken once per day (this may be different for patients who are pregnant or who are being treated for pain).
- Only specialized Opioid Treatment Programs are allowed to treat patients with methadone.
- At the beginning of treatment the patient will typically need to go to the clinic every day to take their daily dose.
- Patients who are making progress in recovery may be provided a supply of medication to take at home.
- Patients should not take more methadone than prescribed or combine methadone with other opioids because of the risk for overdose.
- Many patients will need to continue taking methadone for an extended period of time. Stopping methadone can put the patient at risk for relapse and overdose. This should only be done slowly with careful monitoring by the clinician.
- Treatment with methadone has been shown to reduce the patient’s risk for opioid overdose death.
Naltrexone
- Naltrexone works by blocking opioids from acting on the brain. This means that the patient won’t get high from using opioids while taking naltrexone. Naltrexone is a good option for preventing relapse in patients who are no longer dependent on opioids.
- Patients cannot have any opioids in their body when starting naltrexone. If they do, it will quickly cause severe withdrawal. Before a clinician starts a patient with an active opioid addiction on naltrexone, the patient must go through withdrawal under the clinician’s supervision. This period typically lasts 6–10 days.
- Naltrexone is given in an extended release form that is injected in the buttocks. The injection is administered by the clinician in the office once every 3–4 weeks.
- Naltrexone is also available as a pill, but this form is NOT recommended when treating opioid addiction, except under very limited circumstances.
- Many patients will need to continue taking naltrexone for an extended period of time. Because naltrexone does not produce physical dependence, it can be stopped abruptly without withdrawal symptoms. However, stopping naltrexone can put the patient at risk for relapse and overdose. This should only be done with careful monitoring by the clinician.
HOW DO THESE MEDICATIONS WORK?
Methadone
- Effect: Acts on the same areas of the brain as opioid medications or drugs but with longer lasting effects to stabilize activity in these areas
- Use: Treatment of opioid withdrawal and long-term treatment for opioid addiction
- PROs: Works well to prevent withdrawal, cravings, and use of illicit opioids; reduces risk for opioid overdose death
- CONs:
- Frequent clinic visits
- Can cause overdose if not taken as directed by the clinician
- Risk for overdose when combined with alcohol or sedatives
Buprenorphine
- Effect: Acts on the same areas of the brain as opioid medications or drugs but with longer lasting effects to stabilize activity in these areas
- Use: Treatment of opioid withdrawal and long-term treatment for opioid addiction
- PROs: Works well to prevent withdrawal, cravings, and use of illicit opioids; reduces risk for opioid overdose death
- CONs: Risk for overdose when combined with alcohol or sedatives
Naltrexone
- Effect: Blocks effect of opioids
- Use: Prevent relapse in patients who are no longer dependent on opioids
- PROs: No risk for dependence; reduces cravings
- CONs: Patients are more likely to drop out of treatment with naltrexone
Naloxone
Short-acting effect
- Effect: Blocks effect of opioids
- Use: Treats opioid overdose
- PROs: Saves lives
- CONs: May cause opioid withdrawal symptoms
Medication Use Summary
- Every patient is different. The right medication allows the patient to feel normal, have few side effects, avoid withdrawal symptoms, and have cravings under control.
- When used correctly, and when the treatment plan is being followed, these medications can be taken safely for years.
- Any plans to stop taking a medication, change dosage, or switch medications should always be discussed with the clinician. This should be a shared decision, with all benefits and risks discussed and understood by the patient.
- Patients will often participate in counseling and support groups based on a treatment plan agreed upon by the patient and the clinician. However, participation in counseling and other support services should not be required to receive treatment with medication.
- Relapse may occur as part of this chronic disease. If a patient relapses while using medication, the clinician will work with the patient to revise the treatment plan and treatment goals as needed.
- Naloxone should be administered in the event of a suspected opioid overdose.
Warnings
- Medications kept at home must be locked in a safe place.
- Women should let their clinician know if they are pregnant or breast feeding.
- Combining methadone or buprenorphine with alcohol, sedatives, tranquilizers or other drugs that slow breathing can be deadly.
Pain
- Pain can and should be effectively treated in patients with opioid addiction.
- Methadone or buprenorphine can be effective for treating both opioid addiction and pain.
- The clinician may temporarily increase the patient’s dose, or the frequency of dosing, of methadone or buprenorphine to effectively manage pain.
- The clinician may also prescribe additional pain-relieving medications or other treatments (such as physical therapy).
- Methadone or buprenorphine does not need to be stopped before surgery.
- If methadone or buprenorphine is stopped due to pain treatment, it should be restarted as quickly as possible.
- Naltrexone blocks the action of opioid pain medications. When needed, this blocking effect can often be overcome. In these instances, patients should be closely monitored in an emergency department or hospital setting.
- It is important that patients talk to their clinicians about their opioid addiction and work together to develop a pain management plan that both addresses the pain and minimizes their risk of relapse.
ASSESSMENT AND TREATMENT OF OPIOID USE DISORDER IN PREGNANT WOMEN
- Treatment for opioid use disorder should be initiated as early in the pregnancy as possible.
- Ideally the patient would be seen by a clinician experienced in pregnancy care as well as a clinician experienced in addiction treatment. However, if a specialist is not available, pregnant women should still seek prenatal care and discuss their need for opioid use disorder treatment.
- The clinician should complete a medical evaluation to identify any urgent medical issues that need to be addressed.
- Medical examination can include laboratory tests, physical examination, ultrasound, and questions about the patient’s mental health and individual needs.
- The most important things that a pregnant woman with opioid use disorder can do are to get regular prenatal care and addiction treatment.
- Withdrawal can be dangerous during pregnancy. Patients should work with their clinician to manage withdrawal if they are going to stop or cut down on their opioid use (including prescription opioid use).
- The clinician should talk to the patient about the risks and benefits of the different treatment options. They should make a decision together based on what is best for the patient.
- Methadone and buprenorphine are the best treatments available for pregnant women with opioid use disorder. The clinician may recommend that the patient be hospitalized when the medication is started, especially in the third trimester. However, for most patients these medications can be safely started in an outpatient setting.
- The clinician may also recommend methadone or buprenorphine for pregnant women who are in recovery from opioid use disorder if the patient is at risk for relapse during pregnancy.
- Methadone or buprenorphine are the best options to treat opioid use disorder during pregnancy. However, if the patient is taking naltrexone prior to pregnancy and wants to continue it, the patient should discuss the potential risks with a clinician. Not enough is known about the safety of naltrexone during pregnancy.
- While methadone and buprenorphine have some similarities to other opioids like heroin or oxycodone, their specific properties make them much safer during pregnancy when used under the care of a clinician. These medications are longer acting, preventing opioid withdrawal, opioid overdoses, and the highs and lows that can harm the development of the fetus.
- Later in pregnancy the clinician may increase the dose of medication or have the patient take the medication more frequently to prevent cravings and support a more stable environment for the fetus.
- The clinician may recommend counseling or other behavioral treatments in addition to medication.
- Patients who are taking methadone or buprenorphine as prescribed, and are without other contraindications for breastfeeding, can and should breastfeed.
- After delivery the clinician will evaluate the patient to see if there is a need to adjust the dose of methadone or buprenorphine. Since there is a risk for relapse and overdose in the first year after delivery, patients should typically not stop taking these medications during this time.
FENTANYL: SPECIAL CONSIDERATIONS
- As fentanyl and other high potency opioids have become more common there has been a rapid increase in overdose deaths.
- Patients who have been using fentanyl and similar drugs may have different treatment needs. For example, they may be at risk for more severe withdrawal. They may need a higher level of support to start medication, or they may need a higher medication dose.
- For some patients who have been using fentanyl, It may be more difficult to begin buprenorphine. Their doctor may recommend:
- A more intensive treatment setting, such as residential treatment
- An extended-release formulation of buprenorphine
- Methadone
NALOXONE
ASAM supports broad access to naloxone for individuals commonly in a position to respond to an opioid overdose.
Naloxone (or Narcan) is an important medication for treating an opioid overdose. Everyone who may witness an overdose should have and know how to use this medicine. Encourage friends, family members, and significant others to have naloxone on hand.
HOW TO RECOGNIZE AN OVERDOSE
Someone may be experiencing an opioid overdose if:
- They are unconscious or you cannot wake them.
- Their breathing is slow, irregular, or has stopped (you may hear choking sounds or a gurgling/snoring noise).
- They have pinpoint pupils (their pupils are very small).
- Their fingernails or lips are blue or purple (for darker skinned people the skin may turn pale, grayish, or ashen).
RESPONDING TO A SUSPECTED OVERDOSE
- If overdose is suspected, try to wake the person up by calling their name.
- If that doesn’t work, try grinding your knuckles into the middle of their chest or their upper lip.
- If there is no response, or if you are still unsure of an overdose, call 911 immediately.
- Give naloxone or other overdose reversal medication.
- Support the person’s breathing while you wait for emergency responders. Use CPR if they are not breathing, including providing rescue breaths and chest compressions.
- If breathing, place the person in the recovery position on their side.
- Wait for emergency services to arrive.
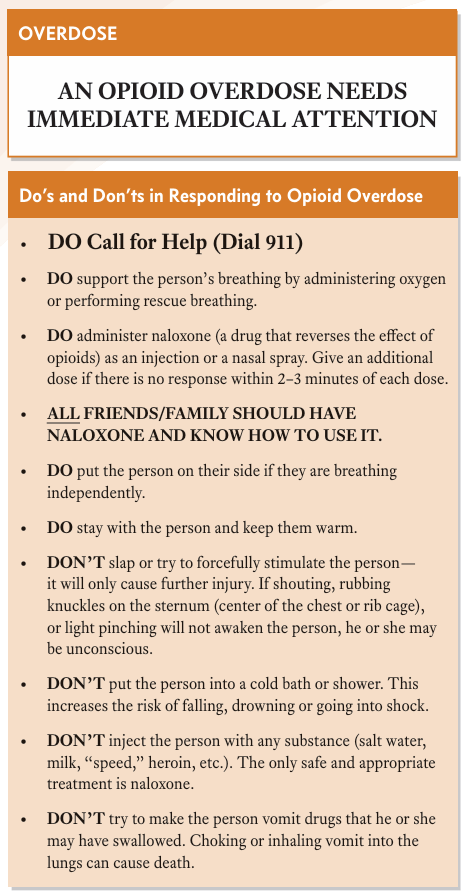
- See “Do’s and Don’ts” for more information.
OVERDOSE
HOW TO GET NALOXONE
You can get naloxone through:
- Naloxone Distribution Programs
- Cost: Free
- Where To Get It: Varies by state. Naloxone is commonly distributed by state and local health departments and harm reduction programs. Search naloxone distribution and [your state] to find locations.
- Over the Counter (OTC)
- Cost: Usually around $50 for two doses
- Where To Get It: Many pharmacies carry naloxone. You can also order online.
- Prescription
- Cost: It depends on your insurance. Some insurance plans may cover all of the cost, while others may require a copay.
- Where To Get It: Ask your doctor for a prescription
Common brand names for naloxone products include: Narcan, Kloxxado, Zimhi, Evzio, RiVive, Rezenopy
OVERDOSE REVERSAL MEDICATION
A new medication, nalmefene, was recently approved by the FDA to treat opioid overdose. However, naloxone is less expensive, more readily available, and currently the preferred medication for reversing an opioid overdose.
Having naloxone available can help to save a person who has taken so much opioid that they stop or have trouble breathing.
If an overdose is suspected, call 911 immediately and give naloxone as soon as possible.
More than one dose of naloxone may be needed to reverse an overdose of high potency opioids, such as fentanyl.
Naloxone may need to be given multiple times since its effects may wear off before the opioid does.
To ensure patient safety, patients, their family members, significant others, and friends should keep naloxone on hand and should be trained in its use in case of overdose.
The clinician should provide naloxone, or a prescription for naloxone, for both the patient and family members. In most states, naloxone is also available without a prescription through the pharmacy.
After patients overdose it is important that they either begin treatment for opioid addiction or work with their clinician to adjust their treatment plan.
QUESTIONS TO ASK YOUR CLINICIAN
- What should I do if I think I have an opioid addiction?
- What types of treatment are available?
- What type of treatment would be best for me?
- How will my treatment change as I make progress in recovery?
- How will you make decisions about changes to my treatment plan, including changes to medications?
- What other services and supports are available to support my recovery?
- Are there differences in cost for treatment medications?
- Does insurance cover the cost of treatment medications?
- Where will I be treated?
- Where can I get naloxone?
Source Citation
The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update. Available at: https://www.asam.org/Quality-Science/quality/ 2020-national-practice-guideline. doi: 10.1097/ADM.0000000000000633
Disclaimer
This resource is for informational purposes only, intended as a quick-reference tool based on the cited source guideline(s), and should not be used as a substitute for the independent professional judgment of healthcare providers. Practice guidelines are unable to account for every individual variation among patients or take the place of clinician judgment, and the ultimate decision concerning the propriety of any course of conduct must be made by healthcare providers after consideration of each individual patient situation. Guideline Central does not endorse any specific guideline(s) or guideline recommendations and has not independently verified the accuracy hereof. Any use of this resource or any other Guideline Central resources is strictly voluntary.
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.