Design and created by Guideline Central in participation with the Consensus and Physician Experts.
Colorectal Cancer Screening Guidelines Toolkit
Consensus and Physician Experts
Publication Date: Mar 5, 2025
Page Last Updated: May 5, 2026
Overview
Background
- In the United States, colorectal cancer (CRC) is the fourth most common cancer diagnosed among adults and the second leading cause of death from cancer.
- In the United States, CRC is most common in adults aged 65 to 74.
- Incidence of CRC (specifically adenocarcinoma) in adults aged 40 to 49 years has increased by almost 15% from 2000-2002 to 2014-2016.In 2016, 25.6% of eligible adults in the US had never been screened for colorectal cancer5 and in 2018, 31.2% were not up to date with screening.
- CRC remains the most preventable, yet least prevented, cancer.
- CRC screening is the process of detecting early-stage CRCs and precancerous lesions in asymptomatic people with no prior history of cancer or precancerous lesions.
- Regular CRC screening may help reduce mortality rates and has the potential to save lives.
- The goal of screening is to reduce overall and cancer-specific morbidity and mortality using strategies that have acceptable harms, burden, and costs.
- The typical pathogenesis of CRC is an adenomatous polyp that slowly increases in size and leads to dysplasia and cancer. Most CRC arises from colonic adenomas. However, 20% to 30% of CRC cases arise through pathways other than the adenoma–carcinoma sequence.
- Progression from adenoma to invasive cancer varies from 5 years or less to more than 20 years. The 10-year cumulative risk for progression to carcinoma is about 10%; some adenomas stabilize and others regress. Progression risk is related to number, size, and histology of adenomatous polyps.
- CRC screening should be performed as part of a population-based program that includes a systematic method for 1) identifying those who are eligible for and wish to undergo screening; 2) risk stratification and administration of the screening tests at agreed upon intervals; 3) shared decision-making with patients regarding the choice of screening method; 4) standardized reporting of the results; and 5) follow-up of those with a positive test. The program should also include a systematic method for the arranging of repeat screening and surveillance.
Abbreviations
- ACG, American College of Gastroenterology
- ACP, American College of Physicians
- ACS, American Cancer Society
- ASCO, American Society of Clinical Oncology
- CRC, colorectal cancer
- CT, computed tomography
- FIT, fecal immunochemical test
- gFOBT, guaiac-based fecal occult blood test
- MACRA, Medicare Access and CHIP Reauthorization Act
- NCCN, National Comprehensive Cancer Network
- sDNA / FIT-DNA test / stool DNA, Cologuard
- USMSTF, US Multi-Society Task Force
- USPSTF, United States Preventive Services Task Force
Guideline Synopsis
Current Guidelines
- There have been over a half dozen clinical practice guidelines published in the United States alone on the topic of Colorectal Cancer Screening.
- The guidelines agree on some points, and disagree or differ on others. There are multiple reasons for differing guidelines, including differences due to:
- Differences in guideline scope — some guidelines focused on average risk only, while others included all patients and risk types.
- Differences in methodology — for example, some guidelines are consensus, others GRADE.
- Age and literature review timelines — spanning 2017 to 2022
- Development from different medical vantage points, from primary care, to oncologists to gastroenterologists, to government agencies.
Current CRC Guidelines Published Since 2018 in the USA
| Organization | Title | Date | Type |
| USPSTF | Colorectal Cancer: Screening | 5/18/2021 | Guideline |
| ACS | Colorectal Cancer Screening for Average-Risk Adults | 5/30/2018 | Guideline |
| NCCN | Colorectal Cancer Screening | 2/27/2024 | Guideline |
| ASCO | Early Detection for Colorectal Cancer | 2/25/2019 | Guideline |
| USMSTF | Age to Start and Stop Colorectal Cancer Screening | 11/15/2021 | Guideline |
| ACG | Colorectal Cancer Screening 2021 | 3/1/2021 | Guideline |
| ACP | Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults | 8/1/2023 | Guideline |
| MACRA | Colorectal Cancer Screening | Ongoing | Quality Measure |
| eCQI | Colorectal Cancer Screening | Ongoing | Quality Measure |
Similarities and Differences
CRC Guideline Similarities
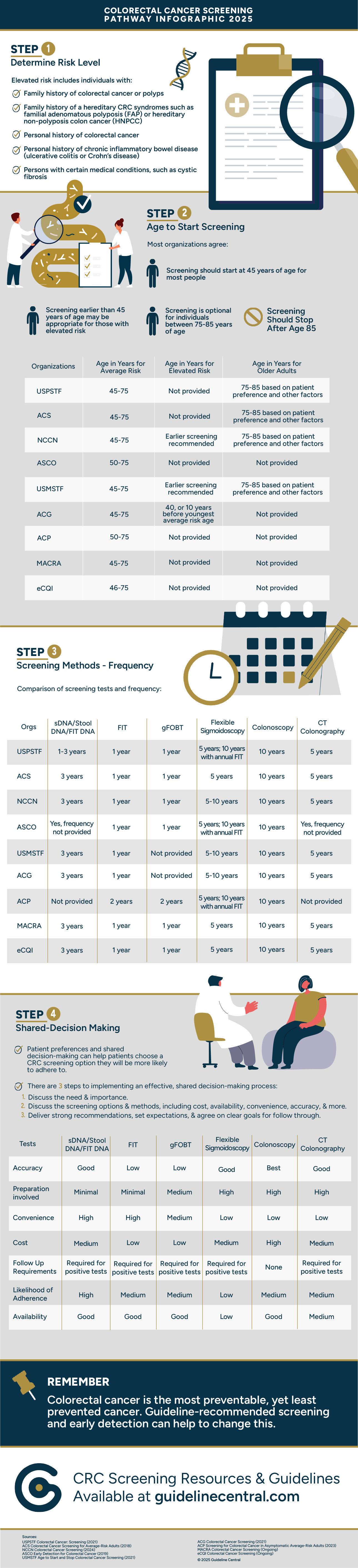
- Most agree that patients younger than 45 should be screened if they are at higher risk for CRC
- Screening can stop at 75 for most patients, and 85 for nearly all patients
- The screening intervals are fairly consistent amongst all guidelines
CRC Guideline Differences
- The newest guidelines recommend that average risk patients should begin screening for CRC at age 45. Only two guidelines recommend starting at 50.
- There is some disagreement on whether there is a first line option - some guidelines say there are preferred tests, while others stress shared decision making between the patient and healthcare provider
Comparison of CRC Screening Guidelines - When to Screen
| Organization | Average Risk | High Risk | Older Adults |
| USPSTF | 45-75 | Not provided | 75-85 based on patient preference and other factors |
| ACS | 45-75 | Not provided | 75-85 based on patient preference and other factors |
| NCCN | 45-75 | Earlier screening recommended | 75-85 based on patient preference and other factors |
| ASCO | 50-75 | Not provided | Not provided |
| USMSTF | 45-75 | Earlier screening recommended | 75-85 based on patient preference and other factors |
| ACG | 45-75 | 40, or 10 years before youngest average risk age | Not provided |
| ACP | 50-75 | Not provided | Not provided |
| MACRA | 45-75 | Not provided | Not provided |
| eCQI | 46-75 | Not provided | Not provided |
Comparison of CRC Screening Guidelines - Tests and Frequency
| Organization | sDNA / Stool DNA / FIT DNA | FIT | gFOBT | Flexible Sigmoidoscopy | Colonoscopy | CT Colonography |
| USPSTF | 1-3 years | 1 year | 1 year | 5 years; 10 year with annual FIT | 10 years | 5 years |
| ACS | 3 years | 1 year | 1 year | 5 years | 10 years | 5 years |
| NCCN | 3 years | 1 year | 1 year | 5-10 years | 10 years | 5 years |
| ASCO | Yes, frequency not provided | 1 year | 1 year | 5 years; 10 year with annual FIT | 10 years | Yes, frequency not provided |
| USMSTF | 3 years | 1 year | Not provided | 5-10 years | 10 years | 5 years |
| ACG | 3 years | 1 year | Not provided | 5-10 years | 10 years | 5 years |
| ACP | Not provided | 2 years | 2 years | 10 years with FIT every 2 years | 10 years | Not provided |
| MACRA | 3 years | 1 year | 1 year | 5 years | 10 years | 5 years |
| eCQI | 3 years | 1 year | 1 year | 5 years | 10 years | 5 years |
USPSTF
Summary of USPSTF Recommendations for CRC Screening
| Population | Recommendation | Grade |
| Adults aged 50 to 75 years | The USPSTF recommends screening for colorectal cancer in all adults aged 50 to 75 years. | A |
| Adults aged 45 to 49 years | The USPSTF recommends screening for colorectal cancer in adults aged 45 to 49 years. | B |
| Adults aged 76 to 85 years | The USPSTF recommends that clinicians selectively offer screening for colorectal cancer in adults aged 76 to 85 years. Evidence indicates that the net benefit of screening all persons in this age group is small. In determining whether this service is appropriate in individual cases, patients and clinicians should consider the patient's overall health, prior screening history, and preferences. | C |
- High-sensitivity gFOBT or FIT every year
- sDNA-FIT every 1 to 3 years
- CT colonography every 5 years
- Flexible sigmoidoscopy every 5 years
- Flexible sigmoidoscopy every 10 years + FIT every year
- Colonoscopy screening every 10 years
Summary of USPSTF Rationale
| Rationale | Adults aged 45-49 y | Adults aged 50-75 y | Adults 76 y or older |
| Detection | • The USPSTF found adequate evidence that screening for colorectal cancer with several different methods can accurately detect early-stage colorectal cancer and adenomatous polyps • Several studies on screening test accuracy include persons younger than 50 y, although few report screening test accuracy specifically for that age group. Those studies that do report accuracy report similar sensitivity and specificity | The USPSTF found convincing evidence that screening for colorectal cancer with several different methods can accurately detect early-stage colorectal cancer and adenomatous polyps | The USPSTF found convincing evidence that screening for colorectal cancer with several different methods can accurately detect early-stage colorectal cancer and adenomatous polyps |
| Benefits of early detection and intervention and treatment | • The USPSTF found adequate evidence that screening for colorectal cancer with stool tests, colonoscopy, CT colonography, or flexible sigmoidoscopy in adults aged 45 to 49 y provides a moderate benefit in terms of reducing colorectal cancer mortality and increasing life-years gained • Although no studies report on the benefits of screening specifically in adults younger than 50 y, some studies reporting an association of fewer colorectal cancer deaths with screening colonoscopy and reduced colorectal cancer mortality with screening gFOBT included patients younger than 50 y • Modeling analyses suggest more life-years are gained and fewer colorectal cancer deaths occur when screening begins at age 45 vs 50 y | The USPSTF found convincing evidence that screening for colorectal cancer with stool tests, colonoscopy, CT colonography, or flexible sigmoidoscopy in adults aged 50 to 75 y provides a substantial benefit in reducing colorectal cancer mortality and increasing life-years gained | The USPSTF found adequate evidence that routine screening for colorectal cancer with stool tests, colonoscopy, CT colonography, or flexible sigmoidoscopy in adults aged 76 to 85 y provides a small to moderate benefit in reducing colorectal cancer mortality and increasing life-years gained |
| Harms of early detection and intervention and treatment | • The USPSTF found adequate evidence that the harms of screening for colorectal cancer in adults aged 45 to 49 y are small. The majority of harms result from the use of colonoscopy (such as bleeding and perforation), either as the screening test or as follow-up for positive findings detected by other screening tests • Although fewer studies include persons younger than 50 y, overall findings suggest risk for bleeding and perforation with colonoscopy and risk for extracolonic findings with CT colonography may be lower at younger ages | The USPSTF found adequate evidence that the harms of screening for colorectal cancer in adults aged 50 to 75 y are small. The majority of harms result from the use of colonoscopy (such as bleeding and perforation), either as the screening test or as follow-up for positive findings detected by other screening tests | • The USPSTF found adequate evidence that the harms of screening for colorectal cancer in adults 76 y and older are small to moderate. The majority of harms result from the use of colonoscopy (such as bleeding and perforation), either as the screening test or as follow-up for positive findings detected by other screening tests • The rate of serious adverse events from colonoscopy and the detection of extracolonic findings on CT colonography from colorectal cancer screening increase with age |
| USPSTF assessment | The USPSTF concludes with moderate certainty that there is a moderate net benefit of starting screening for colorectal cancer in adults aged 45 to 49 y | The USPSTF concludes with high certainty that there is a substantial net benefit of screening for colorectal cancer in adults aged 50 to 75 y | The USPSTF concludes with moderate certainty that there is a small net benefit of screening for colorectal cancer in adults aged 76 to 85 y who have been previously screened |
Screening
Average Risk
- Increasing CRC incidence and mortality, such that incidence rates for 45- to 49-year-olds now matches incidence in populations that are already eligible for average-risk screening. Incidence in 45- to 49-year-olds is similar to the incidence observed in 50-year-olds in 1992 when CRC screening was first recommended for those ages 50 and older. Incidence in all 45- to 49-year-olds is currently similar to incidence in black Americans ages 45 to 49, for whom the MSTF recommended average-risk screening in 2017.
- Emerging data show that the rate of advanced colorectal neoplasia in average-risk individuals ages 45 to 49 is similar to advanced neoplasia rates observed in screening cohorts of those ages 50 to 59.
- Modeling studies that show benefits of screening outweigh harms in average-risk 45-49 year olds. Although not specific to a screening population, data show that colonoscopy is safe in 45- to 49-year-olds.
- Modeling studies demonstrate acceptable cost-effectiveness of average-risk screening to start at age 45.
High Risk
Risk Factors
- Family history of colorectal cancer or polyps
- Family history of a hereditary colorectal cancer syndrome such as familial adenomatous polyposis (FAP) or hereditary non-polyposis colon cancer (HNPCC)
- Personal history of colorectal cancer
- Personal history of chronic inflammatory bowel disease (ulcerative colitis or Crohn disease)
- Persons with certain medical conditions, such as cystic fibrosis
Screening for High Risk
- Initiate colorectal cancer screening with a colonoscopy at age 40 or 10 years before the youngest affected relative, whichever is earlier, in individuals in whom a first-degree relative has had colorectal cancer or an advanced polyp before age 60 years or in whom two or more first-degree relatives have had colorectal cancer or an advanced polyp at any age; perform interval colonoscopy every 5 years.
- Consider initiating CRC screening at age 40 or 10 years before the youngest affected relative, whichever is earlier, for individuals with CRC or advanced polyp in 1 first-degree relative (FDR) at age <60 years or CRC or advanced polyp in ≥2 FDR at any age.
- Consider genetic evaluation with higher familial CRC burden (higher number and/or younger age of affected relatives).
- Consider initiating CRC screening at age 40 or 10 years before the youngest affected relative and then resuming average-risk screening recommendations for individuals with CRC or advanced polyp in 1 FDR at age ≥60 years.
Cystic Fibrosis
- The CF Foundation recommends that CRC screening begin at age 40 y in individuals with CF with continued rescreening every 5 y.
- The CF Foundation recommends that individuals with CF who have undergone a colonoscopy that had any adenomatous polyps have surveillance colonoscopy in 3 y, unless a shorter interval is indicated by individual findings, with subsequent intervals based on the most recent endoscopic examination.
- The CF Foundation recommends that individuals with CF who are 30 years of age and older and have adequately recovered after receiving a solid organ transplantation begin CRC screening within 2 years of transplantation, except when they have had a negative colonoscopy within the past 5 y.
- The CF Foundation recommends continued CRC rescreening every 5 y in individuals with CF who have received a solid organ transplant.
- The CF Foundation recommends that individuals with CF who have undergone a solid organ transplantation and had colonoscopy that had any adenomatous polyps have surveillance colonoscopy in 3 years, unless a shorter interval is indicated by individual findings, with subsequent intervals based on the most recent endoscopic examination.
- The CF Foundation recommends that adults with CF undergoing a colonoscopy receive intensive regimens for bowel preparation to allow for optimal examination. The intensive regimen should include: 3-4 washes (minimum of 1 L purgative per wash) with the last wash occurring within 4-6 h before the examination.
When to Stop Screening
- Given increased competing mortality risks and the increased risk of colonoscopy-associated complications with greater age, the focus of screening among individuals aged 76 to 85 years should be on healthy individuals with no or few comorbidities who are expected to live at least 10 years.
- The decision to screen between ages 76–85 years should be individualized and include a discussion of the risks and benefits based on comorbidity status prior screening history, life expectancy, CRC risk, and personal preference
- Eligible individuals who have not been previously screened are most likely to benefit in this age group.
- Surveillance of individuals between ages 76–85 years should be individualized and include a discussion of risks and benefits of continued colonoscopy based on comorbidity status, estimated life expectancy, and findings on the last or the most recent colonoscopy.
- If there is concern regarding colonoscopy risks, then non colonoscopy options may be preferable. Given the paucity of evidence to inform screening decisions in this age group, patient preference should weigh heavily in the decision.
- Screening is not recommended after age 85.
- After age 85 years, the competing mortality risks and risks of CRC screening complications are sufficiently high that it is reasonable to conclude that the potential harms of screening outweigh the potential benefits in this age group. Consequently, health care professionals should not offer screening to individuals in this age group.
- There may be exceptional circumstances when screening might be considered, such as the individual in excellent health who has not been engaged in routine screening and strongly desires testing; but, in general, screening should be discouraged in individuals older than 85 years.
Tests and Screening Tools
Screening Tests Overview
- The recommendation for CRC screening includes offering patients the opportunity to select either a structural (visual) examination or a high-sensitivity stool-based test, depending on patient preference and test availability.
- Screening options differ in the extent of patient burden and in ways that can affect a patient's choice of test and subsequent adherence, including screening frequency, screening location (home vs medical facility), need for dietary and/or bowel preparation, need for sedation, time and transportation required, relative ability to prevent versus detect CRC, out-of-pocket cost, risk of complications, and test accuracy.
- There is evidence that patients will have a preference for one type of screening test over others if provided sufficient information regarding these test attributes, although no single test appears to consistently dominate patient preferences, supporting a strategy of offering choice.
Recently-Approved Tests and Screening Tools
- Since the initial publication of the CRC Screening Toolkit, multiple new tests and screening tools have been approved by the FDA:
- Cologuard Plus™ (Exact Sciences)
- stool DNA test to screen adults 45 and older at average risk for colorectal cancer
- ColoSense (Geneoscopy)
- multitarget stool RNA (mt-sRNA) test for colorectal cancer (CRC) screening in adults aged 45 or older who are at average risk for CRC
- Shield™ blood test (Guardant Health)
- for colorectal cancer (CRC) screening in adults age 45 and older who are at average risk for the disease
- Cologuard Plus™ (Exact Sciences)
Considerations in Choosing a Colorectal Cancer Screening Test
| TYPE | INTERVAL | LIMITATIONS | PATIENT BURDEN | COST AND REIMBURSEMENT |
| FIT | Annual | • High nonadherence to annual testing (especially in absence of reminder systems) • Less effective for advanced adenoma detection • Few available tests have published peer-reviewed performance data | • Is done at home • Many brands require only a single sample • No diet or medication restrictions | • Inexpensive compared with structural examinations and mt-sDNA • Follow-up colonoscopy for positive test may be subject to out-of-pocket costs |
| gFOBT | Annual | • High nonadherence to annual testing (especially in absence of reminder system) • Less effective for advanced adenoma detection • Difficulty in ascertaining test performance among the many FDA-cleared tests | • Is done at home • Requires multiple samples • Requires dietary and medication restriction • Higher false-positive rate than FIT leads to more colonoscopies | • Inexpensive compared with structural examinations and mt-sDNA • Follow-up colonoscopy for positive test may be subject to out-of-pocket costs |
| sDNA | 1-3 years | • This is a new test, with limited data on screening outcomes, and its performance needs to be monitored over time • There may be uncertainty in management of positive results followed by a negative colonoscopy | • Can be done at home • Does not require bowel preparation, anesthesia or sedation, or transportation to and from the screening examination (test is performed at home) | • More expensive than other stool-based tests • Follow-up colonoscopy for positive test may be subject to out-of-pocket costs |
| Colonoscopy | 10 years | • Risk of bowel perforation/bleeding and cardiopulmonary complications of anesthesia • Performance is dependent upon adequacy of bowel preparation, the cecal intubation rate, withdrawal time, and adenoma detection rate • Limited collection of quality data in many settings • Level of adherence to 10-y interval is unknown • Lower sensitivity for neoplasia in the proximal than the distal colon | • Requires full bowel cleansing • Requires time off work and a chaperone (if sedation is used) | • Most expensive test, but currently reimbursable for those with insurance coverage • Polypectomy and anesthesia may be subject to out-of-pocket costs |
| CT Colonography | 5 years | • Incidental extracolonic findings may require workup, with unclear benefit-burden balance • Exposure to low-dose radiation | • Requires full bowel cleansing • Colonoscopy required if test positive. If same day colonoscopy is not possible, a second bowel cleansing will be required before the follow-up colonoscopy. | • Relatively expensive and may not be covered by insurance (not covered by Medicare at this time) • Follow-up colonoscopy for positive test may be subject to out-of-pocket costs |
| Flexible Sigmoidoscopy | 5-10 years | • Does not examine the proximal colon • Concerns about lack of quality standards, limited availability, failure to achieve a complete examination | • Pain and discomfort • Requires enema prior to procedure • Abnormal findings require second endoscopic procedure (colonoscopy) | • Follow-up colonoscopy for positive test may be subject to out-of-pocket costs |
Shared Decision Making and Adherence
Shared Decision Making Overview
- CRC screening presents a unique challenge and opportunity, as there are multiple screening tests with variability in supporting evidence of effectiveness, risk of harm, prevention potential, and patient burden.
- Shared decision-making can help patients choose a CRC screening option they can adhere to.
- Many organizations recommend that patients be given an opportunity to choose a testing strategy, thus increasing the likelihood of adherence. Patient preference is an important consideration, although the choice of test must be predicated on high-quality screening test options that are accessible to the patient, and there must be access to follow-up colonoscopy if needed.
- There are 3 steps to implementing an effective, shared decision-making process:
- Discuss why a patient fits the criteria for a recommended preventive service
- Communicate available screening options and assess the patient's preferences to find a service they agree to
- Deliver a strong CRC screening recommendation, set patient expectations, and gain patient commitment for follow through
- There is no consistent, direct evidence that adults prefer any one CRC screening tool or strategy over others.
- Individual preferences can be influenced by patient education about screening, test characteristics (ie, accuracy, degree of invasiveness, test preparation, required screening interval, and cost), and clinician recommendation.
SDM Factors to Consider
- Existing conditions
- Family history
- Accuracy
- Preparation involved
- Convenience
- Follow up care
- Cost
- Potential for follow up testing
- Likelihood of Adherence
- Risk
- Availability
Adherence
- Poor utilization of and adherence to CRC screening is a major contributor to avoidable CRC mortality in the United States and has been a persistent challenge since the earliest prospective studies of CRC screening were conducted.
- Optimizing adherence to CRC screening will require a multipronged approach that addresses the barriers to screening at the individual, provider, organizational, and policy levels with evidence-based interventions. Multicomponent interventions to reduce structural barriers have been found to have greater effects on utilization of colonoscopy and FOBT than when single interventions were used.
- We recommend organized screening programs to improve adherence to CRC screening compared with opportunistic screening.
- We suggest the following strategies to improve adherence to screening: patient navigation, patient reminders, clinician interventions, provider recommendations, and clinical decision support tools.
- We suggest the following strategies to improve adherence to follow-up of a positive screening test: Mail and phone reminders, patient navigation, and provider interventions.
- The NCCN CRC Screening Panel recommends the inclusion of mt-sDNA– based testing as a potential screening modality in average-risk individuals. A rescreening interval of every 3 years has been suggested and is approved by the FDA. Using a clinical effectiveness model, one study showed that compared with a 10-year colonoscopy interval, annual mt-sDNA testing resulted in similar decreases in CRC incidence (65% vs. 63%) and mortality (73% vs. 72%).At 3-year intervals, such testing was predicted to reduce CRC incidence and mortality by 57% and 67%, respectively. In addition, there are no or limited data in high-risk individuals who refuse colonoscopy or have limited access to conventional screening strategies; therefore, the use of mt-sDNA–based testing should be individualized in these cases. If the colonoscopy is negative after a FIT or mt-sDNA and no additional symptoms are present, there is no need for further tests.
Barriers for Patients
- Lack of recommendation or referral from PCP
- Fear (usually of colonoscopy)
- Financial struggles
- Lack of support and logistical issues
- The misconception that it is unnecessary for them
- Discomfortable or disgust with the procedure (usually with colonoscopy)
- Unable or unwilling to prep
- Lack of awareness of the need
Description of Tests for Patients
- Several screening tests can be used to find polyps or colorectal cancer. The Task Force outlines the following colorectal cancer screening strategies. It is important to know that if your test result is positive or abnormal on some screening tests (stool tests, flexible sigmoidoscopy, and CT colonography), a colonoscopy test is needed to complete the screening process. Talk to your doctor about which test is right for you.
Stool Tests
- The guaiac-based fecal occult blood test (gFOBT) uses the chemical guaiac to detect blood in the stool.For this test, you receive a test kit from your health care provider. At home, you use a stick or brush to obtain a small amount of stool. You return the test kit to the doctor or a lab, where the stool samples are checked for the presence of blood.
- The fecal immunochemical test (FIT) uses antibodies to detect blood in the stool. It is also done once a year in the same way as a gFOBT.
- The FIT-DNA test (also referred to as the stool DNA test) combines the FIT with a test that detects altered DNA in the stool. For this test, you collect an entire bowel movement and send it to a lab, where it is checked for altered DNA and for the presence of blood. It is done once every three years.
Visual Tests
- Flexible Sigmoidoscopy - For this test, the doctor puts a short, thin, flexible, lighted tube into your rectum. The doctor checks for polyps or cancer inside the rectum and lower third of the colon.
- Colonoscopy - This is similar to flexible sigmoidoscopy, except the doctor uses a longer, thin, flexible, lighted tube to check for polyps or cancer inside the rectum and the entire colon. During the test, the doctor can find and remove most polyps and some cancers. Colonoscopy also is used as a follow-up test if anything unusual is found during one of the other screening tests.
- CT Colonography (Virtual Colonoscopy) - Computed tomography (CT) colonography, also called a virtual colonoscopy, uses X-rays and computers to produce images of the entire colon, which are displayed on a computer screen for the doctor to analyze.
Quality Measures
Title - Quality ID #113 (NQF 0034): Colorectal Cancer Screening (link )
eCQI
Title - Colorectal Cancer Screening (link )
Description
Percentage of adults 45-75 years of age who had appropriate screening for colorectal cancer
Rationale
Colorectal cancer represents eight percent of all new cancer cases in the United States. In 2020, there were an estimated 147,950 new cases of colorectal cancer and an estimated 53,200 deaths attributed to it. According to the National Cancer Institute, about 4.2 percent of men and women will be diagnosed with colorectal cancer at some point during their lifetimes. For most adults, older age is the most important risk factor for colorectal cancer, although being male and black are also associated with higher incidence and mortality. Colorectal cancer is most frequently diagnosed among people 65 to 74 years old (Howlader et al., 2020).
Screening can be effective for finding precancerous lesions (polyps) that could later become malignant, and for detecting early cancers that can be more easily and effectively treated. Precancerous polyps usually take about 10 to 15 years to develop into colorectal cancer, and most can be found and removed before turning into cancer. The five-year relative survival rate for people whose colorectal cancer is found in the early stage before it has spread is about 90 percent (SEER, 2022).
Recommendation Statement
The U.S. Preventive Services Task Force (2021) recommends screening for colorectal cancer in adults aged 45 to 49 years. This is a Grade B recommendation (U.S. Preventive Services Task Force, 2021).
The U.S. Preventive Services Task Force (2021) recommends screening for colorectal cancer in adults aged 50 to 75 years. This is a Grade A recommendation (U.S. Preventive Services Task Force, 2021).
Appropriate screenings are defined by any one of the following:
- Fecal occult blood test (annually)
- Stool DNA (sDNA) with FIT test (every 3 years)
- Flexible sigmoidoscopy (every 5 years)
- Computed tomographic (CT) colonography (every 5 years)
- Colonoscopy (every 10 years)
Guidance
Do not count digital rectal exams (DRE), fecal occult blood tests (FOBTs) performed in an office setting or performed on a sample collected via DRE.
Please note the measure may include screenings performed outside the age range of patients referenced in the initial population. Screenings that occur prior to the measurement period are valid to meet measure criteria.
This eCQM is a patient-based measure.
This version of the eCQM uses QDM version 5.6. Please refer to the eCQI resource center (https://ecqi.healthit.gov/qdm) for more information on the QDM.
Denominator
Equals Initial Population
Denominator Exclusions
- Exclude patients who are in hospice care for any part of the measurement period.
- Exclude patients with a diagnosis or past history of total colectomy or colorectal cancer.
- Exclude patients 66 and older by the end of the measurement period with an indication of frailty for any part of the measurement period who also meet any of the following advanced illness criteria:
- - Advanced illness diagnosis during the measurement period or the year prior
- - OR taking dementia medications during the measurement period or the year prior
- Exclude patients 66 and older by the end of the measurement period who are living long term in a nursing home any time on or before the end of the measurement period.
- Exclude patients receiving palliative care for any part of the measurement period.
Numerator
Patients with one or more screenings for colorectal cancer. Appropriate screenings are defined by any one of the following criteria:
- Fecal occult blood test (FOBT) during the measurement period
- Stool DNA (sDNA) with FIT test during the measurement period or the two years prior to the measurement period
- Flexible sigmoidoscopy during the measurement period or the four years prior to the measurement period
- CT Colonography during the measurement period or the four years prior to the measurement period
- Colonoscopy during the measurement period or the nine years prior to the measurement period
Additional Information
Related Topics
Additional Guidelines
| Organization | Title | Link |
| CF Foundaiton | Cystic Fibrosis Colorectal Cancer Screening | https://www.guidelinecentral.com/guideline/25042/ |
| AGA | Endoscopic Removal of Colorectal Lesions | https://www.guidelinecentral.com/guideline/41949/pocket-guide/560596/ |
| ASCRS | Treatment of Colon Cancer | https://www.guidelinecentral.com/guideline/9106/ |
| ASCO | Late-Stage Colorectal Cancer | https://www.guidelinecentral.com/guideline/7260/ |
| ASCO | Metastatic Colorectal Cancer | https://www.guidelinecentral.com/guideline/2016487/ |
| ASCO | Colorectal Cancer Biomarkers | https://www.guidelinecentral.com/guideline/7434/pocket-guide/8791/ |
| ASCO | Treatment of Patients with Early-Stage Colorectal Cancer | https://www.guidelinecentral.com/guideline/7306/pocket-guide/8169/ |
| ASCO | Adjuvant Therapy for Stage II Colon Cancer | https://www.guidelinecentral.com/guideline/1226271/ |
| USMSTF | Diagnosis and Management of Cancer Risk in the Gastrointestinal Hamartomatous Polyposis Syndromes | https://www.guidelinecentral.com/guideline/1702883/ |
| USMSTF | Endoscopic Recognition and Management Strategies for Malignant Colorectal Polyps | https://www.guidelinecentral.com/guideline/309740/ |
| SAGES | Laparoscopic Resection Of Curable Colon And Rectal Cancer | https://www.guidelinecentral.com/guideline/24498/ |
| ASGE | Role of Endoscopy in the Staging and Management of Colorectal Cancer | https://www.guidelinecentral.com/guideline/9404/ |
| AGA | Bowel Cleansing | https://www.guidelinecentral.com/guideline/7839/ |
| USMSTF | Optimizing Adequacy of Bowel Cleansing for Colonoscopy | https://www.guidelinecentral.com/guideline/7839/ |
| AGA | Follow-Up After Colonoscopy and Polypectomy | https://www.guidelinecentral.com/guideline/41944/ |
Additional Patient Resources
- ACS CancerRisk360 - https://acscancerrisk360.cancer.org/
- Colorectal Cancer Screening (PDQ)—Patient Version - https://www.cancer.gov/types/colorectal
- Colorectal Cancer Screening (PDQ)—Health Professional Version - https://www.cancer.gov/types/colorectal/hp
- Colorectal Cancer Screening Tests - https://www.cdc.gov/cancer/colorectal/basic_info/screening/tests.htm
- The Community Preventive Services Task Force has also issued recommendations on interventions to increase colorectal cancer screening - https://www.thecommunityguide.org/content/task-force-findings-cancer-prevention-and-control.
CRC Screening Toolkit Video
Sources
- https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/colorectal-cancer-screening
- https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21457
- https://www.nccn.org/professionals/physician_gls/pdf/colorectal_screening.pdf
- https://ascopubs.org/doi/full/10.1200/JGO.18.00213
- https://www.giejournal.org/article/S0016-5107(21)01437-1/fulltext
- https://journals.lww.com/ajg/fulltext/2021/03000/acg_clinical_guidelines__colorectal_cancer.14.aspx
- https://www.acpjournals.org/doi/10.7326/m19-0642
- https://qpp.cms.gov/docs/QPP_quality_measure_specifications/CQM-Measures/2023_Measure_113_MIPSCQM.pdf
- https://ecqi.healthit.gov/sites/default/files/ecqm/measures/CMS130v13.html
Video
Infographic
Infographic
Document Overview
- Document Title
- Colorectal Cancer Screening Guidelines Toolkit
- Authoring Society
- Document Publication Date
- Mar 5, 2025
- Page Last Reviewed/Updated
- May 5, 2026
- Document Type
- Other
- Country of Publication
- United States
- Full Text Freely Available
- Yes
- Full Text Guideline
- gastro.org/clinical-guidance/guideline-toolkits/colorectal-cancer-toolkit/
Document Scope, Criteria, and Use Cases
- Document Objectives
The objective of this toolkit is to compare the current guidelines for colorectal cancer screening, and provide a brief synopsis of similarities, differences and key takeaways, It will also serve as a quick-reference tool for other CRC-related resources.
- Scope
- Assessment and Screening, Diagnosis, Management, Prevention
- Diseases/Conditions (MeSH)
D003113 - Colonoscopy
D015179 - Colorectal Neoplasms
D003110 - Colonic Neoplasms
D003113 - Colonoscopy
D015179 - Colorectal Neoplasms
D003110 - Colonic Neoplasms
- Keywords
- CRC, CRC Screening, FIT, advanced adenoma, colonoscopy, colorectal cancer, colorectal cancer screening, sDNA
- Target Patient Population
- All adults
- Target Provider Population
- Internal medicine, family medicine, OBGYN and other allied care providers
- Inclusion Criteria
- Male, Female, Adult, Older Adult
- Health Care Settings
- Ambulatory, Outpatient
- Intended Users
- Nurse, Nurse Practitioner, Physician, Physician Assistant
Guideline Central and select third party use “cookies” on this website to enhance the user experience.
This technology helps us gather statistical and analytical information to optimize the relevant content for you.
The user also has the option to opt-out which may have an effect on the browsing experience.